
Recommended
More Related Content
Similar to abd wall defect mx.pptx
Similar to abd wall defect mx.pptx (20)
Recently uploaded
Recently uploaded (20)
abd wall defect mx.pptx
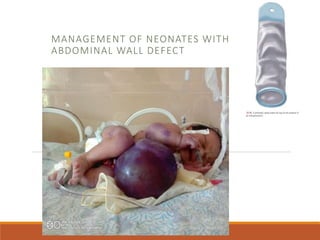
- 1. MANAGEMENT OF NEONATES WITH ABDOMINAL WALL DEFECT
- 2. Outline Prenatal management Postnatal management Research Ethiopia Gastroschisis Primary closure Staged closure Suturless closure Omphalocele Giant omphalocele
- 3. Perinatal management US scanning to look for associated anomalies Delivery route is mainly determined by obstetric indication Usually CS is performed for giant omphalocele Perinatal counseling by multidisciplinary team
- 4. Postnatal management Fluid management For gastroschisis: boluses of 20ml.kg+ high maintenance rate For omphalocele ; 140-150ml/kg/day Hypoglycemia…….beckwith wiedeman syndrome Hypothermia Place the neonate in plastic wrap Put in incubator
- 5. …ctd Decompress abdomen insert NG tube Catheterize Evacuate meconium Start on broad spectrum IV antibiotics Assess the bowel and cover with warm saline soaked gauze
- 7. Over 4 year 39 neonates with AWD : 29 O, 10 G Gastroschisis 90% primary closure, 10% silo/iv bag/ Mortality rate:=70% Omphalocele Conservative with GV :55.2%.......MR =43.3% Primary closure : 37.9%...............MR=25% Staged closure: 6.9%.......................MR=33.3%
- 8. Gastroschisis Primary closure Will be considered In suitable condition Those who came early Easily reducible bowel
- 9. Technique 1) Extend defect vertically 2) Inspect bowel 3) Evacuate meconium 4) Reduce bowel and close abdomen
- 10. Concern in primary closure is the occurrence of ACS ACS occur when Elevated intraabdominal pressure lead to decreased venous return and cardiac output it will result in Hypo perfusion of intraabdominal organs Respiratory :Impaired ventilation and oxygenation
- 12. Measuring intraabdominal pressure Direct way is insert intraperitoneal catheter and connect it to transducer measure pressure Indirect ways intragastic pressure intravesical pressure Peak inspiratory pressure >20mmhg
- 13. Normal IAP is below 10mmhg Indirect measurement of IAP by IVP ,IGP is reliable when PIP and IVP greater than 20 primary closure should be abandoned
- 14. Staged closure with a silo Earlier hand sewn silo bags were commonly used Currently preformed silo bags are available with a ring size of 2-12cm We use urine bag as a silo bag
- 17. 1) suture silo/urine bag to the abdominal wall 2) Dress the silo base with povidone ointed gauze 3) sequentially reduce silo content by twisting Better if reduced within 1 week 4) Take to the OR for closure
- 18. Bianchi suture less closure technique…1998 Elective delayed reduction and no anesthesia Recent cosmetically sound and effective technique Decompress meconium from colon Insert NG tube Wrap bowel with bowel wrap,keep umblical cord long Prepare abdomen with antiseptic
- 19. Give minimal sedation Reduce bowel content slowly and turn by turn over hours Cut umbilical cord long and use that to cover the defect Apply adhesive plaster sutureless closure can also be done with intubation
- 21. Conversion criteria to silo with GA Non reducible matted bowel loop Sign of peritonitis after closure Poor general condition Vital sign derangement with respiratory and circulatory compromise Need for Mechanical ventilator Very narrow defect Major associated anomaly
- 22. Female condom as a silo Used in 20 neonates in Brazil 16 undergo primary closure after 4 days 4 staged closure 1 death due to sepsis from the study
- 24. Intubated vs non intubated 53 neonates undergo suturless umbilical closure 23 non intubated closure attempted : 15 successful ………..1death 8 needs intubation then 6 undergo closure 2 converted to silo 30 intubated suturless closure Both in the intubated and non intubated group rate of complication, need for mechanical ventilation and rate of silo conversion was similar
- 25. Omphalocele Management differs based on the size and associated congenital anomalies Neonatal mortality rate as high as 17-40% depending on associated anomalies reported Initial Work up • Echo for all • Abdominal US • RBS • karyotyping
- 26. Risk factor •Associated anomalies •Size of omphalocele •Respiratory insufficiency ,pulmonary hypoplasia •Rupture of omphalocele sac •Low birth weight ,prematurity •DEFECT size •Presence of rupture
- 27. Immediate repairs For small –medium sized omphalocele Abdominal defect less than 5 cm Those who have good abdominal domain Availability of mesh Stable cardiorespiratory condition
- 28. Primary closure 1) Excision of the sac and skin and fascia closure 2) Reduction 3) Stretch the abdomen manually 4) Reduce midgut followed by liver 5) Leave part of the sac over the liver to prevent hepatic veins injury 6) Leave part of the sac over the bladder 7) Vertical/transverse fascial closure 8) Skin closure and umblicolasty
- 29. Giant omphalocele Defect of 5-6cm ,contains most of the liver Has Mortality rate of 30-46% For giant omphalocele there are two approaches ◦ 1.non operative ◦ 2.operative
- 30. ◦ Primary closure is preferred way of treatment when it is feasible ◦ Omphalocele circumference/abdomen circumference ratio helps to predict success of primary closure ◦ OC/AC ratio of <.26 high chance of primary closure success
- 32. Paint and wait Escharotic therapy Gradual epithelization of omphalocele sac using Povidone iodine Alcohol Mercuchrome Silver sulfidizine,silver nitrate With or without compression
- 33. Indication Chromosomal abnormality Respiratory insufficiency Major associated anomalies Giant omphalocele
- 34. Side effects from scarification treatement Alcohol toxicity Hypothyroidism Silver toxicity: seizure, raised LFT AND RFT, leucopenia Mercury poisoning
- 35. Comparing povidone iodine and Acacia In Egypt they used powder of Acacia niolitica with GV Works by coagulation of protein Make the sac more firm and tough Epithelization completed in 7.8+- 4.8 week Mortality of 25 %
- 37. Comparing saline vs honey Honey is also used as eschcarotic Has no side effect and less rupture and fistula risk Promotes faster healing, full healing 45+-6.8 days # Honey is a good escharotic agent
- 39. 24 NEONATES TOPICAL THERAPY:12.34= -2.12 DAYS NO HYPOTHYRODISIM, NO SAC RUPTURE 6 DEATHS
- 41. Reduction of omphalocele with compression
- 42. Primary closure for large omphalocele In case of difficult fascial closure the following can be used • Skin Flaps • Bridge fascia with mesh • Absorbable, non absorbable,biologic(Gortex,Vicryl,Alloderm) • Component separation • Fascial patch
- 44. Staged closure/Schuster method 1) For a large defect omphalocele with a high volume of eviscerated viscera 2) Excise sac 3) Apply silo: Silastic sheeting is sewn to the fascia/spring loaded silo 4) Serial reduction cutting out a portion of each sheet 5) After full reduction fascial closure or Prosthetic,mesh closure
- 45. USE OF BIOLOGIC MESHS: A STERILE ACELLULAR SHEET DERIVED FROM DERMAL COLLAGEN
- 47. Ventral hernia repair 6mont-1year after Primary fascial closure Component separation Mesh repair
- 48. Component separation technique Degloving of Abdominal skin up to anterior mid axillary line then Fasciotomy to separate External oblique from Rectus abdominus The fasciotomy Will serve as a relaxing incision Rectus abdominus will be sutured at midline
- 50. Prognostic factor >Associated anomalies: cardiac, pulmonary hypoplasia >Giant omphalocele has higher mortality due to the surgical management difficulty >High OC/AC ratio >Liver herniation >Low birth weight, prematurity
- 51. Ruptured Omphalocele Cover the bowel Do silo bag Use of biologic mesh Case reports of successful sac repair
- 52. NEW INNOVATIVE METHOD ◦ Use of tissue expander ◦ Put tissue expanders in the subcutaneous or intermuscular layer ◦ Will result in increase in abdominal capacity
- 53. complication Intestinal obstruction with adhesion Wound infection, dehiscence Neurodevelopmental delay GERD