2.
Understand the basic pathophysiology of CAD
An awareness of the clinical manifestations
An awareness of laboratory findings
Understand the Nursing Management of CAD
◦ Patient Education
◦ Transfusion support and blood warmer
3.
Cold Agglutinin Disease (CAD) is one of the acquired
Autoimmune Haemolytic Anaemias (AIHA). The coldreacting antibodies can lead to premature destruction of
the red blood cells and therefore anaemia.
CAD is rare and has an incidence of 1: 1 000 000 persons.
Predominately found in the female population, and peaks
in the seventh decade of life, however can also be found in
paediatric populations.
Other conditions are sometimes associated with CAD, and
may reflect an underlying malignancy, such as lymphoma,
CLL and Waldenstrom's’ Macroglobinuria.
4.
There are primary and secondary causes of
CAD, however we will focus on the secondary
causes associated CAD.
◦ Secondary causes result from systemic diseases,
which can involve infectious processes or
lymphoproliferative disorders.
◦ CAD can be transient.
5.
Cold agglutinin antibodies occur naturally in
most healthy individuals at low titres. Usually less
than 1:64 at 4°celsius.
Pathological cold agglutinins occur at levels
greater than 1:1000
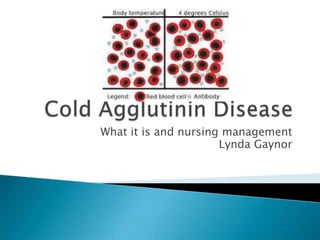
The IgM antibody attaches to the surface of the
red blood cell and causes them to agglutinate, or
clump, at at temperatures below 37°celsius, but
maximally at 0-5°celsius.
6.
This may cause acrocyanosis (impaired blood
flow) to the digits, ears and nose.
8. ◦ Fixation of the complement to the red blood cell by the
cold agglutinin forms the IgM/C3b complement which
coats the red blood cell.
◦ When the IgM/C3b complement circulates to warmer
parts of the body, the IgM dissociates, however the
complement left on the red blood cell can lead to
haemolysis by macrophages in the liver. It is this process
which causes haemolytic anaemia in CAD.
◦ This is usually self-limited as the complement depletes
and so the red blood cell is no longer attractive to the
destructive macrophages.
9.
The next slide is a diagram showing the
mechanism by which the cold agglutinin, IgM
and the complement C3b interact to cause
haemolysis….
11.
Haemolysis can increase during times of
febrile illness as complement levels increase.
Causes of CAD include;
◦ Malignancies, viral infections, genetic abnormalities
eg trisomy 3 and 12, liver transplantation, systemic
sclerosis, malarial splenomegaly, DPT vaccination,
and rarely, patients subjected to hypothermia fir
cardiopulmonary bypass surgery.
12.
For CAD related to infections, there is a good
prognosis if the infection itself is selflimiting. However CAD associated with viral
infections such as HIV has a poorer prognosis
due to the underlying nature of the disease.
A poorer prognosis is also associated with
CAD associated with malignancy.
13. ◦ Anaemia and related symptoms.
◦ Acrocyanosis – 24%
On exposure to cold ambient temperatures, dark,
purple to gray discoloration of the acral (fingers, nose
toes and ears) parts of the body may be noted due to
agglutination. Upon warming, this discoloration will
disappear.
14.
Diagnosis;
◦ Presence of a high titre of cold agglutinins, usually
IgM.
◦ Positive Direct Coombs Test (DAT). This test shows
the presence of antibodies and complement on the
red cell surface.
15.
Avoidance of cold temperatures– this is the
single most useful therapy in CAD.
Cytotoxic agents – including
cyclophosphamide and chorambucil to reduce
the production of antibodies. This is
sometimes used in combination with steroids.
This aggressive treatment is usually used for
patients with an underlying lymphoma.
Rituximab, alone or in combination with
fludaribine for patients with severe
haemolysis.
16.
Plasmapherisis – as an adjunctive therapy to
physically remove IgM antibodies from plasma to
reduce haemolysis. However this treatment is
short lived and is usually used in situations of
severe haemolysis when CAD is due to infection,
to prepare the patient for surgery and severe
Acrocyanosis.
Transfusion support – Interestingly, the
agglutination of the red cells can make it difficult
to determine the ABO type, so ideally the patients
red cells need to be washed with warm normal
saline to remove the IgM antibody in order to
determine the blood type.
19.
Patient Education
◦ Educate the patient about the importance keeping
the body warm by wearing appropriate clothing,
and the avoidance of cold foods and working in
cold areas.
◦ The importance of nutrition, and especially for
maintaining an adequate folic acid intake. It may be
necessary to refer the patient to a dietitian.
◦ Advice patients how to monitor and support for
signs of anaemia.
◦ If patients require cytotoxic/steroid therapy,
educate about the symptoms on how to manage
side effects.
20.
Transfusion support
◦ When transfusing red cells, the use of a blood
warmer is needed if instructed on the “scientific
comment” on the MR17AA at Peter Mac.
21. Blood Warmer
◦ Also refer to Peter Mac Policy on the use of Blood
Warmers (Ref 11.1.1.5) including;
The use of a blood warmer must be documented by a
registered medical officer
As per the guidelines, nursing documentation in the
patient’s medical record should include;
a blood warmer was used, at what temperature and the
the inventory number.
22.
Our blood warmer in MDU and the set
up with the Plum pump as per Beuglar
rep instructions
23.
A link is available with more information abou
the blood warmer below this presentation on
this wikipage .
Any further questions about the blood
warmer, please post/refer to the discussion
page on the wiki page….it is a work in
progress
24. Please add any comments, questions,
suggestions to the discussion page on the wiki space.
And of course, you can ask me as well!
25.
26. Hoffbrand, et al 2001 (4th Ed), Ch.5, Essential
Haematology, Blackwell Science Pty Ltd, Carlton,
Australia
Gertz, M, 2006, Cold Hemolytic
Syndrome,American Society for Haematology, pp
19-23.
Berentsen S, 2011, How I manage cold agglutinin
disease, Br J of Haematology; pp 153-309.
Wendell et al 2013, Clinical features and treatment
of autoimmune hemolytic anemia: Cold
Agglutinins, accessed 1st September 013 from
www. uptodate.com/contents/clinical-featuresand-treatment-of-autoimmune-he
27.
Smeltzer et al 2004, Brunner and Suddarth’s
textbook of Medical-Surgical Nursing 10th Ed,
pp892-893.
Stone, M 2013, Heating up cold Agglutinins,
Inside Blood, 116(17) pp 3119-3120.
Editor's Notes
TheAIHA’s are charactised by a postive DAT, or COOMbs test and divided into warm and cold types includibg warm agglutins and paroxysmal cold haemoglobinuria.
This is mire relevant to our clinical setting
In the test tubes, the one at 37 degrees shows noraml red cells, however at 4 degrees the RBCs have clumped together.The fingers show the consequences of this with the disclouration of the acral parts.
This occurs extravasculary in the liver
Haemolysis inCAD is usually extravascualr where the RBCs are phagocytised by macrophages in the spleen and liver. In CAD thay are predomonatleysequested in the liver
Unlike Reynauds Phenomenon where warming of acral parts can cause reactive hyperemai, or pooling of blood.Acral discoloration can also be produced by placing the patients had in tepid water and slowly adding icePatients may also complain of pain and discomfort on swallowing cold food.