San jacinto eye care technology center wrkup sheet 17
•
1 like•71 views

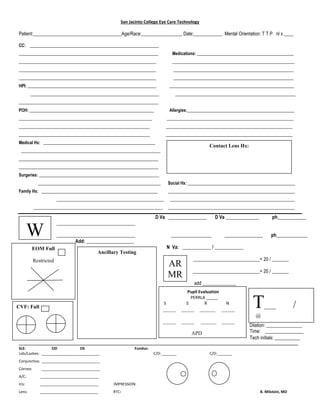
Eye exam form

Recommended
More Related Content
Similar to San jacinto eye care technology center wrkup sheet 17
Similar to San jacinto eye care technology center wrkup sheet 17 (20)
More from Laura Cole, BS, COT, OSC
Recently uploaded
Recently uploaded (20)
San jacinto eye care technology center wrkup sheet 17
- 1. San Jacinto College Eye Care Technology Patient:_____________________________________Age/Race:_________________ Date:____________ Mental Orientation: T T P nl x ____ CC: ____________________________________________________________ _________________________________________________________________ Medications: _____________________________________________ ________________________________________________________________ _________________________________________________________ ________________________________________________________________ ________________________________________________________ ________________________________________________________________ ________________________________________________________ HPI: ____________________________________________________________ __________________________________________________________ ____________________________________________________________ ________________________________________________________ _________________________________________________________________ POH: __________________________________________________________ Allergies:__________________________________________________ ______________________________________________________________ ___________________________________________________________ _____________________________________________________________ ___________________________________________________________ _____________________________________________________________ ___________________________________________________________ Medical Hx: ____________________________________________________ _________________________________________________________________ _________________________________________________________________ _________________________________________________________________ Surgeries: ________________________________________________________ _________________________________________________________ Social Hx: __________________________________________________ Family Hx: ______________________________________________________ ___________________________________________________________ __________________________________________________ __________________________________________________________ ____________________________________________________________ ___________________________________________________________ D Va ________________ D Va ______________ ph____________ _________________________________ _________________________________ _________________ ________________ ph_____________ Add: ____________________ N Va: ____________ / ____________ ____________________________= 20 / _______ ____________________________= 20 / _______ add ______________ Dilation: _______________ Time: ________________ Tech initials: __________ ______________________________________________________________________________________________________________________________________ SLE: OD OS Fundus: Lids/Lashes: ____________________________ C/D: _______ C/D:_______ Conjunctiva: ____________________________ Cornea: ____________________________ A/C: ____________________________ Iris: ____________________________ IMPRESSION: Lens: ____________________________ RTC: B. Milstein, MD W Contact Lens Hx: Pupil Evaluation PERRLA _____ S S R N _____ _____ ______ _____ _____ _____ ______ _____ APD ____ EOM Full Restricted Ancillary Testing T____ / @ CVF: Full AR MR