1. Standardized Patient Modules in Medical School with the
Lesbian, Gay, Bisexual, and Transgender Patient in Mind.
Jacob Anderson, OMS-II; Ashley Jackson, OMS-II; Alexis Stoner, MPH; Ronald Januchowski, DO; Darlene Myles, DO
Acknowledgements: Jennifer Januchowski, RN; Natalie Fadel, PsyD; Renee Prater,
PhD; Reed Allison; Kay Lucas, RN; Ed Magalhaes, PhD; VCOM Institutional Review Board
(James E. Mahaney, PhD, Eryn Perry, Stephanie Hurt); Nelson Sanchez, MD
The Problem
•Disparities in health care needs and access (mental, behavioral, and
physical) exist between cis-gendered heterosexual populations and
the Lesbian, Gay, Bisexual, and Transgender (LGBT) community
(AAMC, 2014).
•Initiatives to decrease health disparities of LGBT patient populations
in the United States have called for an expansion of applicable
research of LGBT populations (IOM, 2011; USDHHS, 2012).
•Among the priority research topics suggested by the IOM,
intervention research is specifically mentioned (IOM, 2011).
•Intervention of medical education curriculum could be of benefit
since, in many schools, only few hours are spent on topics
concerning LGBT health. This includes a lack of case studies that
consider sexual orientation and gender identity (Turbes et al., 2002;
Juno Obedin-Maliver et al., 2011; AAMC, 2014).
•Systematic evaluations of schools that have incorporated LGBT
health studies into their Standardized Patient (SP) evaluations are
limited to a few case studies (Eckstrand et al., 2012; Huang et al.,
2014; Lee and Butterfield, 2014).
Our Study
•Our study was designed to address the problem of potential
exclusivity in medical school curricula by evaluating a Self-Directed
Learning module of LGBT health at Edward Via College of
Osteopathic Medicine (VCOM).
•Measurements were done by comparing results of Attitude Surveys,
Knowledge Surveys, and Sensitive Language Evaluations from SP
encounters. VCOM-Carolinas students served as the exposure group
while VCOM-Virginia served as the control group.
Introduction
Main Objective: to assess the efficacy of LGBT cultural and health
competency learning modules on improving standardized patient
encounters of LGBT patients at a medical school.
1)Can learning modules for medical students increase cultural and
medical competence concerning LGBT patient populations?
2)Can standardized patient encounters be used to effectively
evaluate and improve humanism towards LGBT patient populations?
3)Will this improve the skills of future physicians in a clinical setting?
Methods
Conclusions
Attitudes
Overall, baseline LGBT attitudes scores (max = 65) were similar between
both the Carolinas and Virginia campuses (Carolinas mean +/- se of 48.9
+/- 0.9; and Virginia 41.1 +/- 1.5). Attitude scores did not significantly
change with the intervention (Carolinas 49.4 +/- 0.9), nor in the control
group (Virginia 48.3 +/- 1.7; χ2 = 0.23 , P = 0.63 , DF = 1).
Sensitive Language
Overall, use of the 3 “sensitive language” measures during SP encounters
were similar between both the Carolinas and Virginia campuses (Carolinas
2.2 +/- 0.9; and Virginia 2.7 +/- 0.1). Additionally, use of sensitive language
did not seem to be significantly correlated with a higher attitudes or
knowledge score of individual students on either campus.
1) Subjects from the exposure group (VCOM-CC) and control group (VCOM-
VC) took a pre-survey for qualitative measures of student knowledge and
attitudes regarding LGBT health (Sanchez et al., 2006). Each participating
subject received a random, de-identifying number from the Associate
Dean for Curriculum on each campus, allowing the investigators to link
pre-post test results with SP evaluation results.
2) Students of the exposure group were given access to the "The Sexual
History Examination and the LGBT Patient" self-directed learning module
via email during their reproductive health block of school. The module
consisted of definitions, case-studies, and videos to address health
disparities and sexual history gathering including sexual orientation and
identity (AAMC, 2014).
3) Subjects from the exposure group (N=51) and control group (N=18) were
offered a post-survey with the same questions as the baseline survey to
obtain a comparison of LGBT health knowledge and attitudes between
groups.
4) Standardize Patients evaluated medical students on their sensitivity
during the sexual history examination based on meeting 0, 1, 2, or 3 of
the following criteria (questions from NACHC algorithm, 2014 and
Sullivan et al., 2013):
1) Was gender-neutral language used throughout the SP
encounter?
2) Did the student allow the patient to self-identify their
sexual orientation?
3) If the SP answers “yes” to being sexually active, did the
student ask, “do you have sex with men, women, or both?”
5) Results from the pre-post surveys were matched with SP performance
evaluations and were used to compare the results between campuses as
a whole, and between individual subjects.
Results
Objectives
Results
Discussion
• We found both VCOM campuses scored an average >60% on the attitudes
scale, which agrees with a recent assessment of six other Osteopathic
medical schools (Lapinski et al., 2014) where attitudes tended to be well.
• Similar to assessments of LGBT clinical health knowledge of Medical
Students and Residents; doctors in training tended miss a fair amount of
knowledge-based questions (Sanchez et al., 2006; Lapinski et al., 2014).
• Additionally, our intervention module increased clinical knowledge
unique to LGBT populations.
• The results of our study failed to show that a single module significantly
changed the sensitivity and attitudes of student doctors at VCOM towards
LGBT populations. This may be due to the low participation and high drop-
out rates, however it may reflect a need for integrating LGBT-relevant cases
throughout medical education (Cooke et al., 2010).
• There may have been a degree of selection bias (e.g., students with positive
attitudes chose to participate) and social desirability bias (e.g., students not
answering honestly) present in our study.
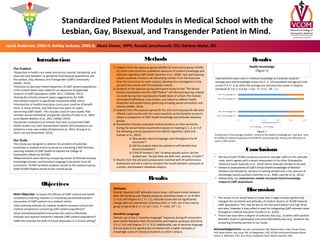
Health Knowledge
(Figure 1)
Improvements were seen in medical knowledge as Carolinas students’
average post-test knowledge scores (10.2 +/- 0.4) exceeded average pre-test
scores (7.9 +/- 0.3), while the average pre and post test scores in Virginia
remained at 7.8 +/- 0.4 (χ2 = 2.61 , P = 0.11 , DF = 1 ).
Figure 1
Comparison of the average students’ scores on the health knowledge pre- and post- tests
at VCOM-CC (exposure group) and VCOM-VC (control group). Passing was defined as a
score ≥ 50% correct.