
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Disorder of adrenal cortex
Similar to Disorder of adrenal cortex (20)
Recently uploaded
Recently uploaded (20)
Disorder of adrenal cortex
- 1. DISORDER OF ADRENAL CORTEX GTJ 320 -- MEDICAL - SURGICAL NURSING III : (Endocrine & Orthopedic Nursing)
- 2. LEARNING OBJECTIVE At the end of this session, I. Student are able to understand etiology and pathophysiology of adrenal cortex disorder II. Identify the clinical manifestation III. Explain the diagnostic investigation related IV. Discuss the treatment, intervention and possible complication V. Apply nursing art / caring value towards patient ~ nursing care
- 3. OVERVIEW OF ADRENAL GLANDS DISORDER It’s condition that interfere with the normal function of the adrenal glands It may cause hyperfunction or hypofunction, and may be congenital or acquired Function of adrenal glands produces hormones that affect growth Development and stress Helps in regulate kidney function Consist of 2 parts adrenal cortex Adrenal medulla Both parts are structurally and functionally different
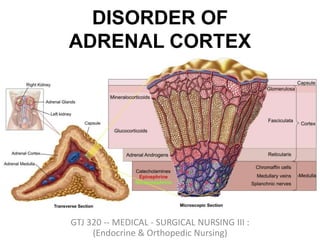
- 5. ADRENAL CORTEX I. Outer part of gland Part of hypothalamus – pituitary – adrenal axis II. Secrete a variety of steriodhormones mineralocorticoids : regulate salt and water balance within the body Glucocorticoids (include cortisol) : wide number of roles within the body Androgens : hormones with testosterone like function
- 6. ADRENAL MEDULLA I. Inner part of gland (20% of gland) Part of sympathetic nervous system 2. Secrete catecholamine's Epinephrine Norepinephrine
- 8. Primary Regulatory Control Anatomy Secretory products Renin-angiotensin Zona glomerulosa Aldosterone ACTH, hypothalamic CRH Zona fasciculata Cortisol and sex hormones ACTH, hypothalamic CRH Zona reticularis Sex hormones (e.g. androgens) Preganglionic sympathetic fibers Medulla Catecholamines (Epi, NE)
- 9. ADRENAL CIRCULATION • Both the left and right adrenals receive arterial blood supply in the same fashion • Paired superior suprarenal arteries - derived from inferior phrenic arteries • Paired middle suprarenal arteries - derived directly from abdominal aorta • Paired inferior suprarenal arteries - derived from the adjacent renal arteries • The left and right adrenals have differing venous drainage • The left adrenal venous drainage is through the left adrenal vein to the left renal vein and finally to the IVC • The right adrenal venous drainage is through the right adrenal vein to the IVC • Recall the same pattern for the left and right gonadal artery/vein
- 10. HISTOLOGY OF ADRENAL GLANDS Adrenal cortex : Arranged in zonal configuration Outer zona glomerulosa = small, compact cells Central zona fasciculata = larger, lipid-rich cells arranged in radial columns Inner zona reticularis = compact & pigmented cells Adrenal medulla Thin layers of large chromaffin cells
- 11. HISTOLOGY OF ADRENAL GLANDS
- 12. FUNCTION OF ADRENAL GLANDS
- 13. REGULATION OF ADRENAL GLAND SECRETION
- 14. ADRENAL CORTEX
- 15. ADRENAL CORTEX • Thelarge cortical cells are arranged into three layers or zones: – Thezona glomerulosa, • Thethin outermost layer • Constitute about 15%of cortex – Thezona fasciculata, • Themiddle and largest portion • Constitute about 75%of cortex. – Thezona reticularis, • Theinnermost zone
- 16. ADRENAL CORTEX • Zonaglomerulosa: – Produce meniralocorticods – Mainly aldosterone (because it containenzyme aldosterone synthase) •Hormones that help control the balance of minerals (Na+ and K+)and water in theblood
- 19. ADRENAL CORTEX • Zonafasciculata: – Produce glucocorticods – Mainly cortisol andcorticosterone – Thehuman adrenal glands produce the equivalent of 35–40 mg of cortisone acetate perday Hormone that play amajor role inglucose metabolism aswell asin protein and lipid metabolism – Thesecretion of these cells is controledby hypothalamic-pituitary axis viaACTH
- 20. ADRENAL CORTEX • Zonareticularis: – Theinnermost layer of the adrenal cortex, lying deep to the zonafaciculata and superficial tothe medulla. – Thesecells produce androgens
- 21. ADRENAL CORTEX • Zonareticularis: –Theandrogens produced includes • Dehydroepiandrosterone (DHEA) • Androstenedione – Synthesized from cholesterol • DHEAis further converted to DHEA- sulfate viaa sulfotransferase
- 22. ADRENAL CORTEX • Zonareticularis: – Theandrogens produced are released into the blood stream and taken up in the testis and ovaries to produce testosterone and theestrogens respectively.
- 23. DISORDER OF ADRENAL CORTEX • Patient with adrenal disorders canpresent with features relatedto: • HYPOFUNCTIONOFTHEGLAND • HYPERFUNCTIONOFTHEGLAND
- 24. TYPES DISORDER OF ADRENAL CORTEX Incidentaloma Primary Hyperaldosteronism Cushing’s Syndrome Adrenocortical Carcinoma Congenital Adrenal Hyperplasia Adrenal Insufficiency
- 26. INTRODUCTION OF ADRENAL HYPOFUNCTION Its a condition in which the adrenal glands are unable to perform well or function less than what they normally should. The causes of adrenal hypofunction are many and include a variety of factors including autoimmune disease. The symptoms of adrenal hypofunction need to be understood well to be able to diagnose and manage the condition. Treatment of adrenal hypofunction is mainly based on its causes and symptoms.
- 27. ADRENAL HYPOFUNCTION • Adrenal insufficiency leads to a reduction in the output of adrenal hormones – glucocorticoids and/or mineralocorticoids • Twotypesof adrenalinsufficiency • Primaryinsufficiency/ Adrenal hypofunction • inability of the adrenal glandstoproduce enough steroid hormones • Secondaryinsufficiency/ Adrenal hypofunction • inadequate pituitary or hypothalamic stimulation of the adrenal glands
- 28. CAUSES OF PRIMARY ADRENAL HYPOFUNCTION Autoimmune disease Genetic diseases Infections Bleeding in glands Surgical removal of adrenal glands
- 29. CAUSES OF SECONDARY ADRENAL HYPOFUNCTION Condition affecting the pituitary gland can cause secondary adrenal hypofunction. The pituitary glands are liable for producing a hormone which conveys message to adrenal gland to produce required cortisol for bodily functioning. If the pituitary gland fails to do this, then no more cortisol will be produced and this causes secondary adrenal hypofunction.
- 30. OTHERS CAUSES OF ADRENAL HYPOFUNCTION -Glucocorticoid treatment – Autoimmune adrenalitis – Tuberculosis – Adrenalectomy – Secondarytumor deposits – Amyloidosis – Haemochromatosis – Histoplasmosis, tuberculosis, CMV, AIDS – adrenal haemorrhage COMMON
- 31. OTHERS CAUSES OF ADRENAL HYPOFUNCTION Metabolic failure in hormone production •Congenital adrenal hyperplasia e.g. 21- hydroxylase deficiency, 3-β-hydroxysteroid dehydrogenase deficiency •Enzyme inhibition e.g. ketoconazole •Accelerated hepatic metabolism of cortisol e.g. phenytoin, barbiturates, rifampicin
- 32. OTHERS CAUSES OF ADRENAL HYPOFUNCTION • Uncommon causes – ACTH blocking antibodies – Mutation in ACTH receptor gene – Adrenal hypoplasia congenita – Familial adrenal insufficiency
- 33. SYMPTOMS OF ADRENAL HYPOFUNCTION Symptoms of adrenal hypofunction mostly based on the deficiency of hormone aldosterone & cortisol High / low blood pressure Low blood sugar level Craving for salty foods Excessive sweating
- 34. SYMPTOMS OF ADRENAL HYPOFUNCTION Unnecessary weight loss Fatigue that becomes worse with passing days Loss of appetite Muscle weakness Irregular or no menstruation in females Headaches.
- 35. ROLES OF HORMONE ALDOSTERONE & CORTISOL To maintain immune system To regulate blood pressure and blood glucose level To maintain salt and electrolytes balance in the body To ensure heart muscles tone and healthy bones To increase body's response to stress.
- 36. LAB TEST FOR ADRENAL HYPOFUNCTION Serum level of cortisol, adrenocorticotropic hormone (ACTH) and Corticotropin-releasing hormone (CRH) ACTH& CRH stimulation test (more specific) X-ray Ultrasound MRI / Ct Scan Detect any changes / problems in adrenal glands or pituitary glands
- 37. TREATMENT FOR ADRENAL HYPOFUNCTION Cortisol replacement steroids therapy Oral replacement (based on height , weight and medication used) Injections (for serious symptoms or adrenal crisis o Only prescribed for emergency situations Specialized diet
- 39. WHAT IS ADDISON’S DISEASE Addison's disease is a disorder that occurs when body produces insufficient amounts of cortisol and often insufficient levels of aldosterone as well. Also called adrenal insufficiency, Addison's disease occurs in all age groups and affects both sexes. Addison's disease can be life-threatening.
- 41. SYMPTOMS OF ADDISON’S DISEASE Extreme fatigue Weight loss & appetite Darkening of your skin (hyperpigmentation) Low blood pressure, even fainting Salt craving Hypoglycemia • Nausea, diarrhea or vomiting • Abdominal pain • Muscle or joint pains • Irritability • Depression • Body hair loss or sexual dysfunction in women Usually develop slowly , often over several months
- 42. ADDISON’S DISEASE : CLINICAL MANIFESTATION • hyperpigmentation
- 43. ADDISON’S DISEASE : CLINICAL MANIFESTATION • hyperpigmentation
- 44. ADDISON’S DISEASE : CLINICAL MANIFESTATION
- 46. ADDISON’S DISEASE : INVESTIGATION Others 1. Complete blood count 2. Blood sugar 3. Urine (routine examination) 4. ECG 5. Chest X-ray 6. Serum electrolytes 7. Bone densitometry 8. Serum creatinine
- 47. ADDISON’S DISEASE : TREATMENT Two main treatment 1. Oral corticosteroids Hydrocortisone (Cortef), prednisone or cortisone acetate may be used to replace cortisol. Your doctor may prescribe fludrocortisone to replace aldosterone. 2. Corticosteroid injection For those not intolerant with oral
- 48. ADDISON’S DISEASE : TREATMENT Replacement of hormones glucocorticoid : hydrocortisone 15mg on waking and 5mg at night Mineralocorticoid : fludrocortisone 0.05mg to 0.1 mg daily Supportive treatment & treatment causes if TB : anti-tubercular therapy
- 49. ADDISON’S DISEASE : TREATMENT General advice to the patient good nutrition : regular meal, high carbohydrate : prevent weight gain sufficient salt : minimize edema and reduce risk for hypertension Diabetic diet : glucose intolerant Administer with meal to prevent ulcer ; When oral therapy is not possible, injection hydrocortisone should be taken. Provide supplementary potassium if possible
- 51. EQYUIVALENT DOSES OF GLUCOCORTICOIDS 1. Hydrocortisone : 20 mg 2. Cortisone acetate : 25 mg 3. Prednisolone : 5 mg 4. Dexamethasone : 0.5 mg
- 53. ADDISON’S DISEASE : COMPLICATIONS Cardiovascular collapse Coma Death
- 54. ADDISONIAN CRISIS Its a medical emergency due to acute adrenocortical insufficientcy
- 55. ADDISONIAN CRISIS : CAUSES Sudden withdrawal of steroid(commonest cause, if pt. on steroid for long time) Following stress e.g.intercurrent disease,trauma, surgery, severe infection or prolonged fasting in a pt with latent insufficiency Following sudden destruction of pituitary gland(pituitary necrosis)or when thyroid hormone or drugs which increase steroid metabolism(e.g. phenytoin)given to a pt with hypoadrenalism Following bilateral adrenalectomy Following injury to both adrenals due to trauma,adrenal vein thrombosis,adrenal haemorrhage due to meningococcaemia or anticoagulant therapy
- 56. ADDISONIAN CRISIS : CLINICAL FEATURES Nausea, vomiting, diarrhea Abdominal pain Diarrhea Muscle cramps Unexplained fever Unconsciousness Severe hypotension Hyponatraemia, hyperkalaemia, hypoglycaemia, hypercalcaemia
- 57. ADDISONIAN CRISIS : TREATMENT I/V hydrocortisone 100 mg 6 hrly until GI symptoms abate then oral therapy I/V fluid normal saline and 10% dextrose for hypoglycaemia Precipitating factors should be find out and treated
- 61. ADDISONIAN CRISIS : DEATH Common causes for death is when patient developed an acute adrenocortical insufficiency and died ~ integrated with other medical problems as example patient may have subclinical hypoadrenalism – increased hepatic metabolism by drug induced
- 62. ADDISON’S DISEASE : NURSING INTERVENTIONS 1. Physical examination Blood pressure (v/sign) Body weight Edema Cataract & glaucoma (3months after treatment) Height ( compression degree of axial spine demineralization)
- 63. ADDISON’S DISEASE : NURSING INTERVENTIONS 2. Coping and support 3. Maintain with follow up / appointment with physician 4. Health education : noted symptoms, make a list of medication, inform family members
- 65. ADRENAL HYPERFUNCTION • It is a condition where there is an overexpression / excessive production of one or more adrenal hormones (aldosterone, corticosteroids, androgenic steroids, epinephrine and norepinephrine). • The increased adrenal gland activity may be caused by an adrenal gland tumor or by excessive stimulation of the gland. Pituitary hormones stimulate adrenal gland activity.
- 66. ADRENAL HYPERFUNCTION There are 3 basic types of corticosteroids elaborated by the adrenal cortex “ glucocorticoids, mineralocorticoids, and sex hormone ” and 4 distinctive hyperadrenal clinical sydromes: • Cushing syndrome : “ excess cortisol ” • Hyperaldosteronism : “ excess aldestrone” • Adrenogenital syndromes : “excess androgen” • Pheochromocytoma : “ high catecholamine”
- 67. HYPERALDOSTERONISM • A medical condition where too much aldosterone is produced by the adrenal glands, which can lead to sodium retention and potassium loss. • Types: –Primary hyperaldosteronism –Secondary hyperaldosteronism
- 68. PRIMARY HYPERALDOSTERONISM Also known as hyporninemic hyperaldosteronism / Conn’s Syndrome
- 69. PRIMARY HYPERALDOSTERONISM / CONN’S SYNDROME 1. Characterized by autonomous excessive production of aldosterone by adrenal glands 2. Presents with hypertension , hypokalaemic alkalosis and renal K+ wasting
- 70. PRIMARY HYPERALDOSTERONISM / CONN’S SYNDROME • Causes: – Adrenal adenoma – Bilateral hypertrophy of zona glomerulosa cells – Adrenal carcinoma •Rare cause
- 71. PRIMARY HYPERALDOSTERONISM / CONN’S SYNDROME • Clinical features: – Hypertension : aldosterone induced Na retention with increase in Extra cellular fluid volume – Muscle weakness: Due to decrease K+ – Muscle paralysis: severe hypokalaemia – Latent tetany (continuous tonic spasm of a muscle; )and paraesthesiae (numbness, itching, and a feeling of pins and needles on your skin) – Polydipsia, polyuria and nocturia: due to hypokalaemic nephropathy
- 72. PRIMARY HYPERALDOSTERONISM / CONN’S SYNDROME Investigation • Electrolyte & blood gasses: – Hypernatraemia – Hypokalaemica – Alkalosis – Urinary potassium loss, level > 30 mmol daily during hypokalaemia
- 73. PRIMARY HYPERALDOSTERONISM / CONN’S SYNDROME Investigation • Plasma aldosterone : renin activity ratio – Sensitive screening test – No need to standardize posture Ratio Interpretation Action <800 Diagnosis excluded Seek other cause >1000,<2000 Diagnosis possible Confirmatory test >2000 Diagnosis very likely Establish cause
- 74. SECONDARY ALDOSTERONISM • Is increased adrenal production of aldosterone in response to non-pituitary, extra-adrenal stimuli • Increase renin secretion – (hyperreninemic hyperaldosteronism) • Commoner than primary aldosteronism
- 75. SECONDARY ALDOSTERONISM Common • CCF • Liver cirrhosis with ascities • Nephrotic syndrome Less common • Renal artery stenosis • Sodium – losing nephritis • Renin—secreting tumours
- 76. CUSHING’S SYNDROME • Adrenal cortex hyperfunction • Any condition resulting from overproduction of primarily glucocorticoid (cortisol) • Mineralocorticoid and androgen may also be excessive
- 78. CAUSES OF CUSHING’S SYNDROME 1. External versus Internal o effect of corticosteroid treatment o asthma and rheumatoid arthritis, or in immunosuppression after an organ transplant. o Over use of medroxyprogesterone acetate 2. Pseudo-Cushing's syndrome
- 79. PSEUDO - CUSHING’S SYNDROME • Appear cushingoid and have some biochemical abnormalities of true Cushing’s disease • Causes – Severe depression – Alcoholism – Obesity – Polycystic ovarian syndrome
- 80. PSEUDO - CUSHING’S SYNDROME : ETIOLOGY • Excessive cortisol (ACTH dependent)~75% • Excessive cortisol (ACTH dependent)~25% • Excess cortisol binding globulin
- 81. PSEUDO - CUSHING’S SYNDROME : ETIOLOGY • Excessive cortisol (ACTH dependent)~75% –Pituitary disease • Adenoma (90%) • Hyperplasia (10 %) –Ectopic ACTH syndrome • Malignancy - ( bronchus, thymus, pancreas, ovary ) –Ectopic CRH syndrome –Exogenous ACTH administration
- 82. PSEUDO - CUSHING’S SYNDROME : ETIOLOGY • Excessive cortisol (ACTH dependent)~25% –Adrenal tumour • Adenoma • carcinoma –Nodular hyperplasia –Exogenous glucocorticoid administration
- 83. PSEUDO - CUSHING’S SYNDROME : ETIOLOGY • Excessive cortisol binding globulin –Estrogen therapy : Osteoporosis, Oral Contraceptic Pill –Pregnancy
- 84. PSEUDO - CUSHING’S SYNDROME : CLINICAL FEATURES • Truncal obesity with deposition of adipose tissue in characteristic site (moon face, buffalo hump)– exact mechanism unknown • Thinning of skin – catabolic response • Purple striae – catabolic response • Excessive bruising – catabolic response
- 85. PSEUDO - CUSHING’S SYNDROME : CLINICAL FEATURES • Hirsutism ( esp adrenal carcinoma ) - ↑ adrenal androgen • Menstrual irregularities - ↑ adrenal androgen • Skin pigmentation ( ACTH ↑ ) – melanocyte stimulating activity
- 86. PSEUDO - CUSHING’S SYNDROME : CLINICAL FEATURES • Hypertension – mineralocorticoid effect → sodium retention – Potassium wasting → hypokalamic alkalosis • Glucose intolerance - ↑ hepatic gluconeogenesis and insulin resistance • Muscle weakness and wasting – catabolic response in peripheral supportive tissue
- 87. PSEUDO - CUSHING’S SYNDROME : CLINICAL FEATURES • Back pain ( osteoporosis and vertebral collapse) – inhibit bone formation • Psychiatric disturbances – euphoria, mania, depression
- 89. PSEUDO - CUSHING’S SYNDROME : LABORATORY INVESTIGATIONS There are two diagnostic steps in the investigation of patient suspected of having Cushing's syndrome Screening test for identification of Cushing's syndrome. the demonstration of high plasma cortisol level Identification of cause
- 90. PSEUDO / CUSHING’S SYNDROME : LABORATORY INVESTIGATIONS 1. Assessment of circadian rhythm in cortisol secretion. Measure 8 am and 11 pm serum cortisol level Normal : Serum value @ midnight is 50% less than value @ 8 am Cushing’s syndrome : rhythum is loss Pseudo-Cushing : normal circadian.
- 91. PSEUDO / CUSHING’S SYNDROME : LABORATORY INVESTIGATIONS 2. Measuring 24-hour urinary free cortisol Level (umol /24 h Interpretation < 300 Normal 300 - 700 Severe depression Stress > 700 Diagnostic of Cushing’s syndrome
- 92. PSEUDO / CUSHING’S SYNDROME : LABORATORY INVESTIGATIONS 3. Low dose Dexamethasone suppression test : 0.5 mg Dexametason (oral) given 6 hourly for 2 days blood for plasma cortisol collected 6 hour after last dose urine for urine free cortisol test(UFC) is collected before & on the 2nd day of Dexa
- 93. PSEUDO / CUSHING’S SYNDROME : LABORATORY INVESTIGATIONS 3. Low dose Dexamethasone suppression test : RESULT UFC suppress by 50% ( < 70nmol/24h Normal plasma cortisol suppress < 140 nmol/L Cushing Pseudo CS no suppression of UFC & Pl. cortisol Cushing’s Syndrome
- 94. PSEUDO / CUSHING’S SYNDROME : LABORATORY INVESTIGATIONS 4. High dose Dexamethasone suppression test : • Normal individuals suppress plasma cortisol to < 50 nmol/L. • Patients with Cushing's syndrome fail to show complete suppression of plasma cortisol levels. This test is highly sensitive (> 97%).
- 95. PSEUDO / CUSHING’S SYNDROME : LABORATORY INVESTIGATIONS 5. Plasma Adrenocorticotropic hormone (ACTH) • Normal < 50 ng/L • Low – adrenal causes • Elevated – Slight – pituitary dependent Cushing’s – Gross – ectopic secretion of ACTH
- 96. PSEUDO / CUSHING’S SYNDROME : LABORATORY INVESTIGATIONS 6. Corticotrophin-releasing hormone (CRH )Test Differentiate ectopic ACTH secretion and Cushing’s disease. Cushing’s disease – plasma ACTH increases 50% over baseline & cortisol increase by 20% Ectopic ACTH or adrenal tumour – no response
- 97. PSEUDO / CUSHING’S SYNDROME : LABORATORY INVESTIGATIONS 7. Imaging CT scan of adrenal gland:TRO adrenal tumor MRI of pituitary gland: majority microadenoma ( < 10mm). MRI reveal lesion in 50 - 60% of cases CT scan/MRI of thorax & abdomen: ectopic ACTH producing tumor
- 98. PSEUDO / CUSHING’S SYNDROME : TREATMENT • Depend of Cushing's syndrome depends on the etiology: – Adrenal adenoma – Adrenal Carcinoma – resection – Cushing’s disease - transphenoidal hyposectomy – Drug ( block cortisol synthesis ) - metyrapone
- 100. PHEOCHROMOCYTOMA • Pheochromocytoma is an extremely rare pathological condition of the adrenal glands where there is development of benign tumors on the cells present in the center of the gland causing symptoms. • The adrenal glands are located at the top of each kidney and are responsible for producing hormones which provide instructions to all the organs and tissues of the body.
- 101. PHEOCHROMOCYTOMA : CAUSES • It’s normally develops in the specialized cells of the adrenal gland called the chromaffin cells. • These cells are located right in the center of the adrenal gland and are responsible for secreting hormones primarily adrenaline. • The hormone adrenaline comes to play when an individual is under stress and calms the body down.
- 102. PHEOCHROMOCYTOMA : CAUSES • This hormone results in an individual having higher blood pressure readings and a fast heart rate. • Pheochromocytoma can causes irregular and excessive release of adrenaline. • Rare but treatable
- 103. PHEOCHROMOCYTOMA : RISK FACTOR • Multiple Endocrine Neoplasia - Type II: This is a disorder in which there is development of tumors in the endocrine system of the body including the thyroid, parathyroid, lips, tongue and the gastrointestinal tract. • Von Hippel-Lindau Disease: This disease can result in development of tumor in the central nervous system, endocrine system, pancreas, and kidneys. • Neurofibromatosis-1: This condition results in development of tumor in the skin and the optic nerve.
- 104. PHEOCHROMOCYTOMA : SYMPTOMS • Some of the most common symptoms of are: –Persistent high blood pressure –Persistent rapid heartbeat –Excessive sweating –Severe / persistent headaches –Tremors –Having a pale face –Shortness of breath.
- 105. PHEOCHROMOCYTOMA : SYMPTOMS • Some of the less common symptoms of are: –Severe anxiety –Abdominal pain –Constipation –Unintentional weight loss.
- 107. PHEOCHROMOCYTOMA : COMPLICATIONS • CNS : stroke secondary to hypertension • CVS : ischemic heart disease (coronary spasm & hypertension), cardiomyopathy (cathecholamines induced myo-necrosis & hypertension) • DM due to insulin antaginsm • Arrhythmia
- 108. PHEOCHROMOCYTOMA : COMPLICATIONS 1- Hormone function: • ECG, ECHO, and blood glucose level. • Suppressor test: clonidine injection iv 5mg → ↓ of BP by 53/25 mmhg for 15 minutes Due to blockade of alpha-receptors in other forms of hypertension but not in Pheochromocytoma.
- 109. PHEOCHROMOCYTOMA : COMPLICATIONS 2- Hormone level: serum catecholamines level is elevated (n=2-5mg/L) neurophysin serum level is elevated (secreted in equimolar concentration with epinephrine)
- 110. PHEOCHROMOCYTOMA : COMPLICATIONS 3. Hormone end product: 24hrs urinary vallinyl mandelic acid (VMA) is elevated Should be collected in acidic medium and refrigerated). The result of the test is falsely high In patients taking alpha-methyl dopa, banana or pine apple (n=2-6 mg/24 hrs).
- 111. PHEOCHROMOCYTOMA : COMPLICATIONS 4- Cause: CT, MRI or sonography of abdomen iodine 131 -metaiodobenzyl guanidine (MIBG) scanning, particularly in extra-abdominal Tumors. Intravenous pyelogram (IVP) may show indentation of the upper pole of kidney
- 113. PHEOCHROMOCYTOMA : TREATMENT • Surgical removal of tumour • Calcium channel blockers control BP • Sympathetic blocking agents – Reduce blood pressure – Reduce symptoms of catecholamine excess • Beta blockers to reduce dysrhythmias • Monitor blood sugar/glucose level
- 114. SUMMARY • The adrenal glands are small glands located on top of each kidney and produce hormones that can't live without, including sex hormones and cortisol. • In adrenal gland disorders, glands make too much or not enough hormones. In Cushing's syndrome, there's too much cortisol, while with Addison's disease, there is too little. Some people are born unable to make enough cortisol.