
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Early Prediction, Proper Planning can lead to Prevention of Disastrous Progression of Uterine Leiomyosarcoma
Similar to Early Prediction, Proper Planning can lead to Prevention of Disastrous Progression of Uterine Leiomyosarcoma (20)
More from Indraneel Jadhav
More from Indraneel Jadhav (13)
Recently uploaded
Recently uploaded (20)
Early Prediction, Proper Planning can lead to Prevention of Disastrous Progression of Uterine Leiomyosarcoma
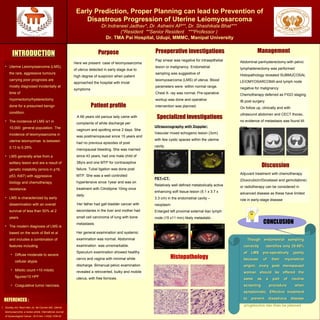
- 1. Early Prediction, Proper Planning can lead to Prevention of Disastrous Progression of Uterine Leiomyosarcoma Dr.Indraneel Jadhav*, Dr. Ashwini AP**, Dr. Shashikala Bhat*** (*Resident **Senior Resident ***Professor ) Dr. TMA Pai Hospital, Udupi, MMMC, Manipal University Purpose ManagementPreoperative investigationsINTRODUCTIONINTRODUCTION Patient profile REFERENCES : REPLACE THIS BOX WITH YOUR ORGANIZATION’S HIGH RESOLUTION LOGO • Uterine Leiomyosarcoma (LMS), the rare, aggressive tumours carrying poor prognosis are mostly diagnosed incidentally at time of myomectomy/hysterectomy done for a presumed benign condition. • The incidence of LMS is1 in 10,000 general population. The incidence of leiomyosarcoma in uterine leiomyomas is between 0.13 to 0.29% • LMS generally arise from a solitary lesion and are a result of genetic instability (errors in p16, p53, Ki67) with aggressive biology and chemotherapy resistance. • LMS is characterized by early dissemination with an overall survival of less than 50% at 2 years. • The modern diagnosis of LMS is based on the work of Bell et al and includes a combination of features including • Diffuse moderate to severe cellular atypia • Mitotic count >10 mitotic figures/10 HPF • Coagulative tumor necrosis. Pap smear was negative for intraepithelial lesion or malignancy. Endometrial sampling was suggestive of leiomyosarcoma (LMS) of uterus. Blood parameters were within normal range. Chest X- ray was normal. Pre-operative workup was done and operative intervention was planned. A 66 years old parous lady came with complaints of white discharge per vaginum and spotting since 2 days. She was postmenopausal since 15 years and had no previous episodes of post menopausal bleeding. She was married since 43 years, had one male child of 38yrs and one MTP for contraceptive failure. Tubal ligation was done post MTP. She was a well controlled hypertensive since 1year and was on treatment with Cilnidipine 10mg once daily. Her father had gall bladder cancer with secondaries in the liver and mother had small cell carcinoma of lung with bone metastasis. Her general examination and systemic examination was normal. Abdominal examination was unremarkable. Speculum examination showed healthy cervix and vagina with minimal white discharge. Bimanual pelvic examination revealed a retroverted, bulky and mobile uterus, with free fornices. 1. Gockley AA, Rauh-Hain JA, del Carmen MG. Uterine leiomyosarcoma: a review article. International Journal of Gynecological Cancer. 2014 Nov 1;24(9):1538-42. Here we present case of leiomyosarcoma of uterus detected in early stage due to high degree of suspicion when patient approached the hospital with trivial symptoms Discussion Though endometrial samplingThough endometrial sampling correctly identifies only 25-50%correctly identifies only 25-50% of LMS pre-operatively (partlyof LMS pre-operatively (partly because of their myometrialbecause of their myometrial origin), every post menopausalorigin), every post menopausal woman should be offered thewoman should be offered the same as a part of routinesame as a part of routine screening procedure whenscreening procedure when symptomatic. Effective treatmentsymptomatic. Effective treatment to prevent disastrous diseaseto prevent disastrous disease progression can then be plannedprogression can then be planned CONCLUSION Specialized investigations Ultrasonography with Doppler: Vascular mixed echogenic lesion (3cm) with few cystic spaces within the uterine cavity. PET–CT: Relatively well defined metabolically active enhancing soft tissue lesion (5.1 x 3.7 x 3.3 cm) in the endometrial cavity – neoplasm Enlarged left proximal external iliac lymph node (15 x11 mm) likely metastatic . Abdominal panhysterectomy with pelvic lymphadenectomy was performed Histopathology revealed SUBMUCOSAL LEIOMYOSARCOMA and lymph node negative for malignancy Chemotherapy deferred as FIGO staging IB post surgery On follow up, clinically and with ultrasound abdomen and CECT thorax, no evidence of metastasis was found till date Adjuvant treatment with chemotherapy (Doxorubicin/Docetaxel and gemcitabine) or radiotherapy can be considered in advanced disease as these have limited role in early-stage disease Histopathology