More Related Content
Similar to SURF Poster (20)
SURF Poster
- 1. RESEARCH POSTER PRESENTATION DESIGN © 2011
www.PosterPresentations.com
New Biokinetics Approach for Determining Plutonium and
Americium
The ability to predict the exposure of specific organs or tissues to
radioactivity, and the excretion of radioactivity from the body, is
key to understanding the health effects of accidental exposure to
radionuclides. The aim of this study is to present an alternate,
simplified model of plutonium (Pu) excretion from the analysis of
well-documented Pu-infected cases involving repeated diethylene-
triamine-penta-acetic acid (DTPA) Three modeling approaches
were simultaneously applied involving: (1) release of soluble Pu
from the wound into the systemic circulation, estimated with a
dissolution model, (2) systemic disposition of Pu with a classic
model, as compared to two alternative models recently reported
and (3) additional “Pu-DTPA” compartments which transfer Pu
directly to urinary compartment from blood, interstitial fluids and
liver. Model simulations were compared to biological data . Results
indicated that inclusion of three DTPA compartments provided
reasonable prediction for Pu and Am distribution into human
organs. However, additional data will be required in other to fully
elaborate a predictive model for Pu exposure in individual human
tissues.
ABSTRACT
INTRODUCTION
Modeling approaches
The first approach involved the dissolution of Pu and its transfer
from the wound to the blood. For this purpose, the simplest
dissolution model of ICRP 66 has been applied, assuming that the
whole dissolved fraction moved directly to the blood. In this
model, a fraction of the initial radionuclide deposit dissolved
quickly at a daily rate. The second one described the behavior of
Pu after systemic contamination according to three different
models: the model currently in use which is described in ICRP 67,
and two other models recently reported.
The last approach described the formation of Pu-DTPA and the
biological behavior of this complex. For this purpose, virtual DTPA
compartments were considered which transfer Pu directly to urine
from body fluids and from the wound. The following assumptions
were applied for modeling: (1) 90% of Pu in the body fluids formed
DTPA complexes, but this chelating process is limited to 2 h after
the beginning of the perfusion, (2) when no direct decorporation
of the wound occurred, after each DTPA treatment, the amount of
Pu-DTPA generated from the wound corresponds to 90% of the daily
dissolution rate. Once the modeling approach provided results in
agreement with bioassay data, the fits between the simulations
and these data can be improved by assuming that a fraction of the
Pu retained in the liver can be decorporated. Such assumption is
supported by bioassay data reported after human contamination
by americium.
This biokinetic modeling will be completed by dose calculations
performed according to ICRP recommendations of ICRP 60. Thus,
committed doses can be calculated taking into account or not the
DTPA treatments, which provides an estimate of DTPA efficacy in
terms of diminution of equivalent and effective doses.
Modelling Pu decorporation by DTPA
The simulated curve of Pu urinary excretion after DTPA treatments
is close to the biological data up to 20 d after contamination. At
the other times, the increased Pu excretion induced by DTPA is
systematically underestimated. By contrast, a good fit is observed
for the excretion measured at a delay longer than 1 d after
treatment except between days 20 and 60. A third-DTPA
compartment was considered to improve the fit of simulations to
biological data. With the ICRP 67 model, a good fit is obtained for
urine excretion up to 20 d after the contamination. However, an
underestimate by a factor of about 2 is systematically observed for
urine samples collected for 24 h after treatments from day 25 to
day 390. Such an underestimate was not observed by using the two
other systemic models. In the case of Luciani's model, the urinary
excretion of Pu is underestimated by a factor of about 2 for times
later than 400 d, which was not observed using the Leggett's
model. Thus, this last model appears to be the most suitable for
analysis of bioassay data obtained after DTPA treatments.
However, a significant underestimate of urinary excretion is
observed between days 20 and 60. Nearly perfect fit could be
obtained between days 20 and 390, assuming that 30% of the liver0
compartment (in the Leggett's model, three liver compartments
are considered) or of the liver1 (in the ICRP 67 and Luciani's
models, two liver compartments are considered) is decorporated
after each DTPA treatment at times less than 100 d, and only 3%
Material and Methods later on. Similar results were obtained for the ICRP 67 model
assuming a liver decorporation of 50 and 15%, respectively.
However, such large efficacy in liver decorporation appears
unrealistic.
Figure 2. Best fit of simulations to biological data after application
of ICRP 67 model assuming the presence of two DTPA
compartments. Squares, wound retention; closed circles, urine
samples collected for the first 24 h after DTPA treatments; open
circles, urine samples collected later on; bolt line, simulation for
Pu retention in the wound; normal line, simulation of daily urinary
excretion of Pu. Data collected from Leggett et al.
Data analysis
Calculations have been performed to estimate treatment benefits
in term of doses, assuming no efficacy of the DTPA treatments.
Similar equivalent and effective doses are obtained after the
application of the three systemic models. The dose delivered to
the wound might be much larger and its diminution associated
with the DTPA treatments cannot be assessed. For such doses, the
ICRP recommendations used to assess tumour occurrence are not
applicable. To our knowledge, no blood data has been reported in
workers after wound contamination by transuranium elements.
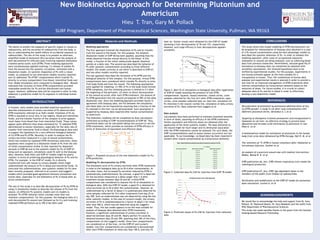
Figure 3. Collected data Pu-238 for injection from ICRP 78 model
Figure 4. Predicted values of Pu-238 for injection from collected
data
CONCLUSIONS
This study shows that simple modeling of DTPA decorporation can
be proposed for interpretation of bioassay data obtained in a case
of a Pu wound contamination using the best physiologic models to
described the systemic behaviour of Pu. In order to validate this
modeling approach, other cases of occupational exposures
(inhalation or wound) are being analysed, such as collecting blood
data from previous researches. Nevertheless, because good fits of
simulations to bioassay data can sometimes be obtained with
unrealistic assumptions, the retained hypotheses have to be
verified by experimental studies. For this purpose, experiments in
non-human primates appear as the most suitable for a
transposition to human. Thus, the combination of human data
analyses and experimental results is planned in order to provide a
new tool for an improved management of DTPA treatments after
internal contamination by transuranium elements based on the
reduction of doses. For future studies, it is crucial to collect
adequate data of Pu and Am in blood in order to effectively
develop a new biokinetics model.
REFERENCES
Decorporation of plutonium by pulmonary administration of dry
Ca-DTPA powder: a study in rat after lung contamination with
different plutonium forms. Sérandour A. L et al
Targeting of diethylene triamine pentaacetic acid encapsulated in
liposomes to rat liver: an effective strategy to prevent bone
deposition and increase urine elimination of plutonium in rats.
Phan G. et al
A mathematical model for estimation of plutonium in the human
body from urine data influenced by DTPA therapy. Hall R. M. et al
The retention of 14C-DTPA in human volunteers after inhalation or
intravenous injection. Stather et al
An analysis of a puncture wound case with medical intervention.
Radiat. Bailey B. R. et al
ICRP publication 66, Ann. ICRP, Human respiratory tract model for
radiological protection.
ICRP publication 67, Ann. ICRP, Age dependent doses to the
members of the public from intakes of radionuclides.
Verification and modification of the ICRP-67 model for plutonium
dose calculation. Luciani A. et al
ACKNOWLEDGEMENTS
We would like to acknowledge the help and support from Dr. Gary
Pollack, Dr. Raymond Quock, Dr. Gary Meadows and the staffs from
WSU Department of Pharmaceutical Sciences.
This study was made possible thanks to the grant from the Summer
Undergraduate Research Fellowship.
In humans, early studies have provided empirical equations to
describe enhancement of urinary excretion of Pu observed after
DTPA treatments referred to as Hall's model. Chelation of Pu by
DTPA is assumed to occur only in two regions, blood and interstitial
fluids, and the transfer fraction of the complex to urine appears
much faster from blood than from interstitial fluids. These values
appear quite different than those estimated for 14C-labelled DTPA
administered to human volunteers, especially for the daily rate of
transfer from interstitial fluid to blood. No physiological data exist
to support the hypothesis for a very different biological behavior
of Ca-DTPA and Pu-DTPA. Recently, in order to analyze the Pu
urinary excretion measured in a case of wound contamination,
which was treated by repeated DTPA intravenous injections, these
equations were coupled to a dissolution model of Pu from the site
of initial contamination similar to that reported for deposited
aerosols in ICRP 66 and to the systemic model for Pu of ICRP 67.
Using such an approach, simulations could fit well to the bioassay
data. However, both Hall's and ICRP 67 models might be poorly
realistic in terms of predicting physiological behavior of Pu and Pu-
DTPA. For example, in the ICRP 67 model, Pu is directly
transferred from soft tissues to urinary bladder which might
underestimate the amount of Pu in blood and interstitial fluids. To
overcome this underestimation, new systemic models for Pu have
been recently proposed, referred to as Luciani's and Leggett's
models which provided good agreement between simulations and
human data, especially for the biokinetics of Pu in blood after an
acute contamination.
The aim of this study is to describe decorporation of Pu by DTPA by
using (1) dissolution models to describe the release of Pu from the
wound, (2) different Pu systemic models and (3) models to
simulate ‘Pu-DTPA’ behavior which consider more than two
retention compartments. For this purpose, the biological data of a
well-documented Pu wound case followed up for 8 y and involving
repeated DTPA perfusions up to 390 d has been used
Figure 1. Proposed structure of the new biokinetics model for Pu-
DTPA prediction.
SURF Program, Department of Pharmaceutical Sciences, Washington State University, Pullman, WA 99163
Hieu T. Tran, Gary M. Pollack
0.00E+00
1.00E-03
2.00E-03
3.00E-03
4.00E-03
5.00E-03
6.00E-03
7.00E-03
8.00E-03
9.00E-03
0 2 4 6 8 10 12
BqperBqintake
Days
Predicted Values of Pu-238 (injected)
Urinary Excretion
facecal Excretion
Table 1. Special Monitoring: predicted values (Bq per Bq intake) for injection of Pu-238
f1 = 5.0E-04
Time after intake (d) Daily urinary excretion Daily faecal excretion
1 8.20E-03 1.60E-03
2 4.50E-03 4.30E-03
3 2.60E-03 4.20E-03
4 1.70E-03 3.10E-03
5 1.20E-03 2.20E-03
6 8.90E-04 1.50E-03
7 6.70E-04 1.00E-03
8 5.30E-04 7.10E-04
9 4.20E-04 5.00E-04
10 3.50E-04 3.60E-04