1. 4. Con base en el artículo Effects of coenzyme Q10
supplementation on oxidative stress and antioxidant enzyme
activity in glazers de Maryam Hormozi y cols. 2018,
conteste lo que se le solicita a continuación:
1. ¿Qué diseño se utilizó en este estudio?
2. ¿Cuál es el objetivo del estudio?
3. ¿Qué tipo de cegamiento se llevó a cabo y en qué consistió?
4. ¿Qué tipo de aleatorización se llevó a cabo y qué fortalezas
brinda?
5. Mencione cuál fue la variable independiente principal, describa
cómo se operacionalizó.
6. ¿Cuáles fueron las covariables que se midieron en el estudio?
7. ¿Cuál es la razón por la que se eligieron esos criterios de
exclusión?
8. ¿De cuánto fue el periodo de seguimiento?
9. Mencione cuál fue el evento de interés o variable dependiente,
describa cómo se definió.
10. ¿Cuál es la población a la que se pueden extrapolar los
resultados del estudio?
11. ¿Cuál es la finalidad de presentar los resultados de la Tabla
2?
12. Describa 2 ventajas al utilizar este diseño en para probar
esta hipótesis.
13. ¿Identifica algún sesgo de selección?, ¿Por qué?, en caso
de que sí, ¿Cómo podría evitarlo/disminuirlo?
14. ¿Identifica algún sesgo de confusión?, ¿Por qué?, en caso de
que sí, ¿Cómo podría evitarlo/disminuirlo?
15. ¿Cuál fue la utilidad principal de los resultados del estudio?
3. Keywords
Coenzyme Q10, oxidative stress, cadmium, antioxidants, malondialdehyde
Received 6 May 2018; Revised 11 August 2018; Accepted 28 August 2018
Introduction
Cadmium (Cd) is an industrial and environmental
contaminant, mainly resulting from battery, electro-
plating and pigment industries, and smoking (Stohs
and Bagchi, 1995). Glazers are highly exposed to
this toxic metal in tile-glazing industry (Hormozi
et al., 2018; Shouroki et al., 2015). Cd affects the
biological system by directly increasing reactive
oxygen species (ROS) and diminishing antioxidant
reserves, especially the enzymes (Valko et al., 2005;
Wang and Fowler, 2008). This toxic metal alters
cellular membranes, resulting in oxidative damage
of lipids, proteins, and DNA. It also causes various
pathological conditions like hepatic and renal
impairment, testicular damage, and respiratory as
well as neurological disorders (Joseph, 2009;
Thompson and Bannigan, 2008).
It has been demonstrated that various antioxidants
and the enzymatic antioxidant defense system (e.g.
superoxide dismutase (SOD), catalase (CAT), and
glutathione peroxidase (GPx)) protect cells against
Cd-induced toxicity (Tandon et al., 2003). In fact,
by directly quenching free radicals and chelating toxic
metals, antioxidants can affect biological systems
(Flora et al., 2013). There is evidence that oxidative
stress, as a major mechanism, plays a primary role in
Cd-mediated cytotoxicity (Cuypers et al., 2010; Ercal
et al., 2001). Coenzyme Q10 (CoQ10) or ubiquinone
is an endogenous lipid-soluble antioxidant and an
integral component of the mitochondrial electron
transport chain (Bhagavan and Chopra, 2006).
Besides, it is helpful in preventing lipids, protein, and
DNA oxidation as it can be continuously regenerated
by intracellular reduction systems (Crane, 2001). In
oxidative stress models, coenzyme Q10 treatment has
been shown to preserve mitochondrial membrane
potential and reduce ROS levels by free radicals-
scavenging (Somayajulu et al., 2005). It has also been
reported to exhibit protective effects against oxidative
damage induced by Cd in rats pretreated with coen-
zyme Q10 (Ognjanović et al., 2006, 2010). Multiple
studies have affirmed the protective effect of coen-
zyme Q10 on oxidative stress in patients with heart
failure, Parkinson’s disease, neurodegenerative, and
hypertensive diseases (Fotino et al., 2013; Rosenfeldt
et al., 2007; Seet et al., 2014; Spindler et al., 2009).
However, there is scant evidence confirming the ben-
eficial impact of coenzyme Q10 against Cd toxicity.
To the best of our knowledge, this is the first study to
examine the effect of coenzyme Q10 on Cd-induced
oxidative stress in occupationally exposed workers.
Exposure to Cd is associated with elevated oxidative
stress, and treatment with antioxidants like coenzyme
Q10 with few side effects has become increasingly
popular (Young et al., 2012). Therefore, this research
has been designed to evaluate the protective effects of
coenzyme Q10 supplementation on lipid peroxidation
and antioxidant enzymes activity in Cd-exposed
glazers. This is a double-blind, placebo-controlled,
2-month crossover clinical trial.
Materials and methods
Subjects
A total of 40 male glazers with occupational exposure
to Cd levels (ranging from 3.82 to 13.81 mg/L in
blood) and an average of exposure history of
6.70 + 0.39 years were enrolled in the study. Subjects
with a history of hypertension, diabetes, and liver,
renal, thyroid and cardiovascular diseases within the
previous 12 months or those who had taken antioxi-
dant vitamin supplements including coenzyme Q10
were excluded. Information on the absence of disease
history was collected using the medical records
obtained from the results of laboratory tests which
had been conducted on the subjects. These tests were
annually performed by the physician of occupational
medicine in the tile industry. Glazers were asked not
to change their usual diets and physical activities dur-
ing the interventional period. The age, smoking habit,
alcohol consumption, body mass index (BMI), and
blood pressure (BP) of glazers were recorded at the
beginning of the study. Weight and standing height of
the participants were measured; then, the BMI was
calculated as kilograms per meter squared. BP of each
subject was measured by the trained assistant using
digital monitoring after at least 5 min of rest in
the sitting position. The average of three BP
2 Toxicology and Industrial Health XX(X)
4. measurements at 2-min intervals was considered as
the final BP values.
Study design
This study was designed as a randomized, double-
blind, placebo-controlled 2-month crossover study,
with 1-month washout period between intervention
phases. Participants were composed of all the glazers
who were working at least 1 year or more before
beginning of the study from tile-glazing industries
in Birjand city, the east of Iran, during 2017. The
study protocol was approved by the Ethics Committee
for Medical Research of Zahedan University of
Medical Sciences, Zahedan, IR Iran (No.
IR.ZAUMS.REC.85.5-June-2016) and registered
with the Iranian Registry of Clinical Trials (No.
IRCT2016061228407N1).
Informed consent. All the participants gave written
informed consent to participate in the study.
Randomization
Randomization was performed through minimizing
smoking, BMI, and age variables by the fifth author
who had no clinical involvement in the trial. The eli-
gible subjects were then assigned to one of the two
study groups of placebo and treatment with coenzyme
Q10 supplementation (60 mg twice daily) for
2 months. After a 1-month washout period, the sub-
jects received the alternative treatment for a further
2 months. Both coenzyme Q10 (manufactured in
Canada) and placebo (starch) were supplied by a phar-
maceutical company (Zahravi, Tehran, IR Iran) and
obtained in identical matching capsules in appear-
ance. The coenzyme Q10 and placebo capsules were
packed in identically coded pillboxes without any
other character mark. They were administered daily
by an independent health expert who was unaware of
the assignment of treatment. Side effects were
assessed using self-reported surveys of glazer’s feel-
ings. The participants and investigators administering
the intervention were blind with respect to group
assignment. The dose (60 mg twice daily) used in this
study for a 2-month period was almost the same as the
treatment dose and period adopted in a clinical trial to
assess the efficacy of coenzyme Q10 in the treatment
of the disease associated with oxidative stress (Lee
et al., 2012).
Blood sampling
Blood samples of each subject were taken at the base-
line, at the end of the first intervention period, after
the washout, and then after the second intervention
period to measure the MDA levels and antioxidant
enzymes activity of SOD and GPx in serum. The
venous blood specimens (10 mL) were collected at
the beginning of the work shift according to the stan-
dard procedure using gel-containing tubes without
anticoagulant by a trained technician. After coagula-
tion, samples were centrifuged at 3500 g/10 min for
separation the serum. Then, serum samples were
divided in aliquots and stored at 70
C until the anal-
ysis time. In order to assess the blood Cd levels, 1 mL
of the whole blood from all the glazers was collected
in heparinized blood collection tubes and stored at
4
C until analyzed.
Cd concentration assay
The Cd levels in whole blood (Cd-B) were measured
using a Perkin Elmer Analyst 700 (Perkin Elmer,
Waltham, Massachusetts, USA) graphite furnace
atomic absorption spectrometer and graphite Mass
man cuvette, with the absorbance measurement at
wavelength ¼ 228.8 nm. Preparation of the samples
was done according to the method given by Andresen
(1986). In this method, the samples were diluted to
1:5 with a surfactant solution containing 0.1% Triton
X-100 (v/v) in deionized water. Blood Cd concentra-
tion was expressed as microgram per liter.
Lipid peroxidation assay
Serum MDA concentration was determined spectro-
photometrically by measuring the thiobarbituric acid
reactive substances, according to the method of
Uchiyama and Mihara (1978). In this method, an ali-
quot 3 mL of 1% phosphoric acid and 1 mL of 0.6%
thiobarbituric acid solution w/v was added to 0.5 mL
of serum. The mixture was heated for 45 min in a
boiling water bath. After cooling, mixture was centri-
fuged at 3000 g/10 min, and the absorbance of
supernatant was measured at ¼ 535 nm against a
blank sample. The results were expressed as micro-
moles per liter in serum.
Total antioxidant capacity assay
The assessment of total antioxidant capacity (TAC)
level in serum was carried out by the method of
Benzie and Strain (1999). Totally, 1.5 mL of working
Hormozi et al. 3
5. ferric reducing–antioxidant power reagent (25 mL 0.3
M sodium acetate buffer, pH 3.6; 2.5 mL 0.01 M
tripyridyl-triazine in 0.04 M hydrochloric acid;
2.5 mL 0.02 M FeCl36H2O; preheated to 37
C) was
mixed with 50 mL of serum; the absorbance was
measured at ¼ 593 nm after a 5-min incubation at
37
C. Ferrous sulfate solutions were used for calibra-
tion. Concentration of TAC was expressed as micro-
moles per milliliter in serum.
Antioxidant enzymes activity assays
The activity of antioxidant enzymes of SOD, GPx,
and CAT in the serum of glazers were measured using
commercially available assay kits (ZellBio GmbH,
Germany, Cat No. ZB-96A) according to the manu-
facturer’s instructions. The absorbance of SOD, GPx,
and CAT were read with an ELISA reader at wave-
lengths of 420, 412, and 405 nm, respectively. Activ-
ity of these enzymes was expressed as unit per
milliliter in serum.
Biochemical parameters
The hemoglobin level in erythrocytes was determined
using flow cytometry method and analyzed by high-
pressure liquid chromatography. The hematocrit was
calculated from the complete blood cell count using the
Coulter impedance principle by automatic cell count
analyzers. These blood parameters were performed by
a trained operator in a hematology laboratory.
Outcome measures
The primary outcomes were 2 months changes in
mean MDA and TAC levels, and the activities of
SOD, GPx, and CAT between coenzyme Q10 and
placebo groups. The other outcomes were 2 months
the difference in mean the serum levels of MDA, TAC
and the activities of SOD, GPx, and CAT from base-
line within each group.
Sample size
To determine the sample size, the changes from
baseline between coenzyme Q10 and placebo were
expected to be 3.0 + 3.0 mmol/L of serum for MDA
levels; hence, the power was set at 80% to detect a
statistically significant difference with type I error
probability of 0.05 (two-tailed ¼ 0.05). The min-
imum sample size achieved was 11 in each group.
Considering the loss to follow-up during phases of
the intervention, a total of 40 glazers in a crossover
design were enrolled in this study (20 subjects in
each group).
Statistical analyses
Statistical analyses were carried out using SPSS Base
version 17.0 for Windows (SPSS, Chicago, Illinois,
USA). Quantitative variables were expressed as mean
+ standard error of mean (SEM). The normal distri-
bution of quantitative variables was tested by the Sha-
piro–Wilk test. Repeated measures analysis of
variance (ANOVA) was employed for comparison
of changes from baseline of each outcome, between
placebo and coenzyme Q10 groups in the crossover
design. Treatment sequences were also randomized
independently for each participant to examining the
order effect. To investigate the basic hypothesis of
crossover design, the absence of a carry-over effect
was detected for each of the outcomes. p Values less
than 0.05 were considered statistically significant.
Results
Overall, 40 male glazers, aged 25–44 years, with
occupational Cd exposure (mean ¼ 8.90 + 0.44 mg/L)
were entered in the study. All subjects completed the
study and were included in the analysis (Figure 1).
Demographic characteristics and some of the basic
blood parameters of enrolled subjects are shown in
Table 1. Approximately 5% of the glazers (two
subjects) were smokers, and none of the subjects
studied consumed alcohol. At baseline, the two
study groups were balanced for all the investigated
variables before coenzyme Q10 and placebo inter-
vention phases. With respect to age, BMI, BP, and
smoking habit at baseline, there were no statisti-
cally significant differences between the coenzyme
Q10 (n ¼ 20) and placebo (n ¼ 20) groups (data
not shown).
The effect of the coenzyme Q10 supplementation
on MDA as a marker of lipid peroxidation and TAC
as well as antioxidant enzymes activity of SOD,
GPx, and CAT are shown in Figures 2 and 3,
respectively.
Lipid peroxidation
There was a significant reduction in the mean serum
MDA levels of glazers following coenzyme Q10
administration compared with placebo (F (1, 38) ¼
85.04, p 0.001). Furthermore, in the coenzyme Q10
supplemented group, the MDA levels were
4 Toxicology and Industrial Health XX(X)
6. significantly less than baseline values (5.51 + 0.26
vs. 6.86 + 0.29 mmol/L) after a 2-month coenzyme
Q10 intervention (Table 2).
Total antioxidant capacity
There were no significant effects of coenzyme
Q10 on the mean serum TAC levels of glazers in
comparison to placebo treatment (F (1, 38) ¼ 2.91,
p ¼ 0.096), although there was a small decrease in
the TAC levels during placebo administration
(Table 2).
Antioxidant enzymes activity
There was a significant increase in the mean activity
of SOD (F (1, 38) ¼ 30.34, p 0.001) and GPx (F (1,
38) ¼ 2.11, p ¼ 0.003) in serum of glazers during
coenzyme Q10 supplementation compared with pla-
cebo. While, there was a significant decrease in the
mean activity of CAT (F (1, 38) ¼ 96.83, p 0.001)
during coenzyme Q10 versus placebo treatment
(Table 2).
Compared to baseline values, glazers in the pla-
cebo group had significantly lower SOD (30.70 +
0.82 vs. 27.30 + 0.88 U/mL of serum) and GPx
(134.47 + 5.27 vs. 127.53 + 6.19 vs. U/mL of
serum) activities, as well as higher CAT activity
(15.70 + 0.97 vs. 16.68 + 1.05 U/mL of serum).
Furthermore, the glazers in the coenzyme Q10 group
had significantly higher activities of SOD and GPx
than at baseline after the 2-month intervention. The
treatment order interaction effects were not signifi-
cant for all responses (p 0.05), suggesting that there
was no order effect in the design. In addition, a review
of the profile plots of repeated measure ANOVA sug-
gested that there was no carry over effect of benefits
from initial administration of the treatment.
Tolerability and adverse events
In this trial, no serious adverse effects were
reported during either coenzyme Q10 or placebo
Figure 1. Flow diagram of glazers through the trial study.
Table 1. Baseline characteristics of the glazers enrolled in
the trial (n ¼ 40).a
Glazers characteristics Mean + SEM
Age (years) 31.83 + 0.79
BMI (kg/m2
) 23.93 + 0.52
Job experience (years) 6.70 + 0.39
Smoking; number (%) 2 (5.0)
Blood Cd (mg/L) 8.90 + 0.44
Hemoglobin (g/dL) 15.12 + 0.17
Hematocrit (%) 44.61 + 0.52
Systolic BP (mmHg) 110.50 + 1.53
Diastolic BP (mmHg) 71.84 + 1.21
SEM: standard error of mean; BMI: body mass index; BP: blood
pressure; Cd: cadmium.
a
Data are represented as mean + SEM.
Hormozi et al. 5
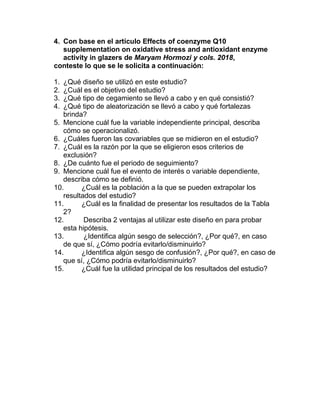
7. Figure 3. (a) Antioxidants serum levels of SOD (units per milliliter), (b) CAT, and (c) GPx (units per milliliter) in the two
intervention groups. SOD: superoxide dismutase; CAT: catalase; GPx: glutathione peroxidase.
Figure 2. (a) Serum levels of TAC (micromoles per milliliter) and (b) MDA (micromoles per liter) in the two intervention
groups. TAC: total antioxidant capacity; MDA: malondialdehyde.
6 Toxicology and Industrial Health XX(X)
8. supplementation except for two subjects who reported
mild headache in the coenzyme Q10 group. Although
some of the hematology safety data were not mea-
sured during the coenzyme Q10 administration, mul-
tiple studies (Baggio et al., 1994; Feigin et al., 1996;
Ferrante et al., 2005; Ikematsu et al., 2006; Rosenfeldt
et al., 2007; Shults et al., 2004; Storch et al., 2007;
Young et al., 2012) have reported that coenzyme Q10
is a well-tolerated and safe supplementation. Further-
more, this supplementation was not clinically associ-
ated with significant changes in safety parameters
even at higher doses in the present study.
Discussion
The present study was designed to determine whether
coenzyme Q10 supplementation at a dose of 120 mg/
day could be beneficial in protecting glazers against
Cd-induced stress oxidative. It was observed that,
compared to placebo, 2 months of coenzyme Q10
supplementation was associated with a significant
reduction in serum MDA levels. Thus, coenzyme
Q10 at a dose of 60 mg twice daily significantly
decreased lipid peroxidation in glazers. Consistent
with these results, pretreatment with coenzyme Q10
(20 mg/kg body weight) has been shown to exert a
protective effect against Cd-induced oxidative dam-
age by reducing lipid peroxidation (MDA) in the
testes (Ognjanović et al., 2010) and the blood of
Cd-treated rats (Paunović et al., 2017). The findings
of the current research also concord with other rando-
mized, placebo-controlled studies that have demon-
strated that coenzyme Q10 supplement, compared
with placebo, significantly decreased lipid peroxida-
tion (MDA) and reduced oxidative stress in patients
with coronary artery disease (Lee et al., 2012) and
nonproliferative diabetic retinopathy (Rodrı́guez-
Carrizalez et al., 2016).
Numerous studies in animal models (Casalino
et al., 2002; Ognjanović et al., 2003; Patra et al.,
1999) and occupational studies (Babu et al., 2006;
Bizon et al., 2013; Garçon et al., 2004; Sciskalska
et al., 2014) have observed a relationship between
Cd exposure and increased MDA levels. Coenzyme
Q10 can produce rapid protective effects against lipid
peroxides (MDA) (Ernster and Dallner, 1995), indi-
cating free radical-induced damage during Cd intox-
ication (Casalino et al., 2002; Waisberg et al., 2003).
The serum TAC provides a complete panorama of
the function of antioxidant system in the body under
oxidative stress (Rodrı́guez-Carrizalez et al., 2016). It
has been revealed that exposure to trace elements
such as Cd, lead, aluminum, arsenic, and mercury
could reduce the level of TAC in the body. More
recently, the authors have noted that Cd-induced
stress oxidative is associated with decreased TAC
levels in serum of glazers, compared to control sub-
jects (Hormozi et al., 2018).
In the present study, although there was a small
increase in TAC levels in favor of coenzyme Q10,
these effects were not statistically significant. This
indicates that 2-month coenzyme Q10 administration
does not contribute to the serum TAC level in Cd-
exposed glazers.
Diminished activities of SOD, GPx, and CAT have
been reported in both occupational studies (Babu
et al., 2006; Bizoń and Milnerowicz, 2014; Moitra
et al., 2014; Nzengue et al., 2011) and in different
tissues of Cd- treated rats (Ognjanović et al., 2010;
Ogunrinola et al., 2016; Oyinloye et al., 2016;
Paunović et al., 2017). The interaction between Cd
and essential trace elements could be one of the
Table 2. Effect of coenzyme Q10 on lipid peroxidation, TAC and antioxidant enzymes activity (n ¼ 40).a
Variables
Coenzyme Q10 Placebo
Mean difference of changesb
p Valuec
Baseline 2 months Baseline 2 months
MDA 6.86 + 0.29 5.51 + 0.26 6.69 + 0.26 6.90 + 0.29 1.55 (1.89, 1.21) 0.001
TAC 1.04 + 0.03 1.06 + 0.04 1.07 + 0.04 0.99 + 0.03 0.10 (0.03, 0.22) 0.096
SOD 30.75 + 0.97 33.94 + 1.09 30.70 + 0.82 27.30 + 0.88 6.59 (4.20, 8.98) 0.001
GPx 128.13 + 5.66 145.61 + 7.10 134.47 + 5.27 127.53 + 6.19 24.42 (9.24, 39.60) 0.003
CAT 17.92 + 1.06 11.21 + 0.99 15.70 + 0.97 16.68 + 1.05 7.69 (9.27, 6.12) 0.001
MDA: malondialdehyde (mmol/L); TAC: total antioxidant capacity (mmol/mL); SOD: superoxide dismutase (U/mL); GPx: glutathione
peroxidase (U/mL); CAT: catalase (U/mL); SEM: standard error of mean; ANOVA: analysis of variance.
a
Data are represented as mean + SEM.
b
Difference between mean change after coenzyme Q10 and placebo (95% CI).
c
ANOVA with repeated measures for comparison of between group changes. Statistical significance was considered as p 0.05.
Hormozi et al. 7
9. reasons for decreased activity of antioxidant enzymes
(Ognjanović et al., 2010).
In a previous study, the authors observed a distur-
bance in the serum levels of antioxidants by a signif-
icant reduction in the activities of SOD and GPx and a
significant increase in the CAT activity of
Cd-exposed glazers, compared with the controls
(Hormozi et al., 2018). Increased activity of CAT in
glazers may be due to the direct enzyme activation by
Cd as a consequence of overproduction of ROS and
the compensatory mechanism developed to balance
the excess of lipid peroxidation.
In the current study, treatment with coenzyme Q10
clearly entailed a significant increase in the activity of
SOD and GPx and a significant decrease in the CAT
activity, compared with the placebo group. Indeed,
alterations occurred in the activity of antioxidant
defense enzymes since Cd-induced toxicity had been
prevented through treatment with coenzyme Q10.
Up-regulating the activities of SOD, GPx, and
CAT is consistent with previous studies that reported
a significant reduction in the activities of SOD, CAT,
and GPx in various tissues of Cd-treated rats. On the
other hand, pretreatment with coenzyme Q10 (20 mg/
kg body weight), as a potent antioxidant, provided a
protection against Cd-induced oxidative stress by
enhancing the activity of these enzymes in rat tissues.
Moreover, the authors found a more protective impact
of coenzyme Q10 in Cd-treated rats when adminis-
tered in combination with vitamin E (Ognjanović
et al., 2010; Paunović et al., 2017).
The results of this research also in agreement with
randomized, parallel, placebo-controlled studies that
demonstrated the effects of 12 weeks coenzyme Q10
supplements (150 and 300 mg/day) on antioxidant
enzyme activities through increasing the activities of
SOD (Lee et al., 2012, 2013) and GPx (Lee et al.,
2013) in coronary artery disease patients. However,
this suggestion is in contrast with those studies claim-
ing that coenzyme Q10 supplementation is associated
with decreased GPx activity (Rodrı́guez-Carrizalez
et al., 2016) and/or that it has no effect on GPx activ-
ity (Lee et al., 2012). This inconsistency may be
owing to differences in both the dose used and the
treatment period. In this regard, it has been suggested
that the coenzyme Q10 administered at higher doses
(300 mg/day) has better antioxidative effects than
when prescribed at lower doses.
Antioxidant enzymes (e.g. SOD, GPx) are the
potential targets of Cd and are regarded as the first
line of defense against ROS (Flora et al., 2013). The
inhibition of their activities contributes to the rise of
oxidative stress in Cd toxicity (Brzóska et al., 2016).
However, the activity of these enzymes heightens
immediately after antioxidant supplementation (Khar-
aeva et al., 2009).
Coenzyme Q10 has an important role in preventing
lipid peroxidation and protecting tissues against oxi-
dative damage. In fact, by scavenging ROS, coen-
zyme Q10 can be indirectly involved in regulating
the gene expression and modulating the activities of
most enzymes. Thus, this antioxidant may alter the
activity of many enzymes, especially oxidative dam-
age repair enzymes (Tiano et al., 2012).
On the other hand, it has been established in
numerous experimental models that under intoxica-
tion with Cd, the concentration of vitamins E and C
reduces in the blood and various tissues (Ognjanović
et al., 2010, 2006; Paunović et al., 2017). Neverthe-
less, coenzyme Q10 has been reported to enhance
cellular antioxidant defense mechanism via other
pathways; these include recycling and regenerating
endogenous antioxidants such as vitamins C and E
(Arroyo et al., 2004; Beyer, 1994; Lass and Sohal,
2000; Ognjanović et al., 2010).
In the present study, the authors investigated the
impact of the oxidized form of coenzyme Q10 (ubi-
quinone), because it is more commonly available on
the market as a dietary supplement. The International
Coenzyme Q10 Association has suggested 300 mg/day
of coenzyme Q10 supplements for healthy adults.
However, there are no recommended doses for coen-
zyme Q10 supplements in Iran.
Concerning the limitations of this study, it has to
be mentioned first that the researchers did not exam-
ine the values of nonenzymatic antioxidants (e.g.
reduced glutathione (GSH), as well as vitamins C
and E). However, Paunović et al. (2017) documented
that administration of coenzyme Q10 under acute
intoxication with Cd significantly improves the lev-
els of these antioxidants in the blood. Second, this
study was designed based on 120-mg coenzyme Q10
supplements for only 2 months. These results can be
further confirmed in larger and longer trials and/or
by combining coenzyme Q10 with other antioxidants
such as vitamin E.
In conclusion, the results suggest that coenzyme
Q10 supplementation (120 mg /day) may potentially
protect glazers against Cd-induced oxidative stress
both by reducing lipid peroxidation and by improving
antioxidant enzymes activity. Thus, coenzyme Q10
can be considered as a promising agent for further
8 Toxicology and Industrial Health XX(X)
10. investigation in terms of its efficacy to protect work-
ers who are under chronic exposure to Cd.
Acknowledgments
The authors would like to thank the managers and workers
of tile factories for their kind cooperation. Also, the writers
are grateful to the management of Zahravi Pharmaceutical
Company for its collaboration in preparing the placebo.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest
with respect to the research, authorship, and/or publication
of this article.
Funding
The author(s) disclosed receipt of the following financial
support for the research, authorship, and/or publication of
this article: This study was supported by a dissertation grant
(PhD thesis, no.: project: 7615) to first author from Zahe-
dan university of Medical Sciences, Zahedan, Iran.
ORCID iD
Maryam Hormozi http://orcid.org/0000-0001-6064-3
196
References
Andresen BD (1986) Textbook of Clinical Chemistry.
London: Saunders Company.
Arroyo A, Rodrı́guez-Aguilera JC, Santos-Ocaña C, et al.
(2004) Stabilization of extracellular ascorbate mediated
by coenzyme Q transmembrane electron transport.
Methods in Enzymology 378: 207–217.
Babu KR, Rajmohan HR, Rajan BK, et al. (2006) Plasma
lipid peroxidation and erythrocyte antioxidant enzymes
status in workers exposed to cadmium. Toxicology and
Industrial Health 22(8): 329–335.
Baggio E, Gandini R, Plancher AC, et al. (1994) Italian
multicenter study on the safety and efficacy of coen-
zyme Q10 as adjunctive therapy in heart failure. CoQ10
Drug Surveillance Investigators. Molecular Aspects of
Medicine 15: 287–294.
Benzie IF and Strain JJ (1999) Ferric reducing/antioxidant
power assay: direct measure of total antioxidant activity
of biological fluids and modified version for simulta-
neous measurement of total antioxidant power and
ascorbic acid concentration. Methods in Enzymology
299: 15–27.
Beyer RE (1994) The role of ascorbate in antioxidant pro-
tection of biomolecules: interaction with vitamin E and
coenzyme Q. Journal of Bioenergetics and Biomem-
branes 26(4): 349–358.
Bhagavan HN and Chopra RK (2006) Coenzyme Q10:
Absorption, tissue uptake, metabolism and pharmacoki-
netics. Free Radical Research 40(5): 445–453.
Bizoń A and Milnerowicz H (2014) Participation of metal-
lothionein and superoxide dismutase in the blood of
smoking smelters. International Journal of Occupa-
tional Medicine and Environmental Health 27(2):
326–334.
Bizon A, Antonowicz-Juchniewicz J, Andrzejak R, et al.
(2013) The influence of the intensity of smoking and
years of work in the metallurgy on pro- oxidant/antiox-
idant balance in the blood of smelters. Toxicology and
Industrial Health 29(2): 149–161.
Brzóska MM, Borowska S and Tomczyk M (2016) Anti-
oxidants as a potential preventive and therapeutic strat-
egy for cadmium. Current Drug Targets 17(12):
1350–1384.
Casalino E, Calzaretti G, Sblano C, et al. (2002) Molecular
inhibitory mechanisms of antioxidant enzymes in rat
liver and kidney by cadmium. Toxicology 179(1–2):
37–50.
Crane FL (2001) Biochemical functions of coenzyme Q10.
Journal of the American College of Nutrition 20(6):
591–598.
Cuypers A, Plusquin M, Remans T, et al. (2010) Cadmium
stress: an oxidative challenge. Biometals 23(5):
927–940.
Ercal N, Gurer-Orhan H and Aykin-Burns N (2001) Toxic
metals and oxidative stress part I: mechanisms involved
in metal-induced oxidative damage. Current Topics in
Medicinal Chemistry 1(6): 529–539.
Ernster L and Dallner G (1995) Biochemical, physiological
and medical aspects of ubiquinone function. Biochimica
et Biophysica Acta (BBA)-Molecular Basis of Disease
1271(1): 195–204.
Feigin A, Kieburtz K, Como P, et al. (1996) Assessment of
coenzyme Q10 tolerability in Huntington’s disease.
Movement Disorders 11(3): 321–323.
Ferrante KL, Shefner J, Zhang H, et al. (2005) Tolerance
of high-dose (3,000 mg/day) coenzyme Q10 in ALS.
Neurology 65(11): 1834–1836.
Flora SJ, Shrivastava R and Mittal M (2013) Chemistry and
pharmacological properties of some natural and syn-
thetic antioxidants for heavy metal toxicity. Current
Medicinal Chemistry 20(36): 4540–4574.
Fotino AD, Thompson-Paul AM and Bazzano LA (2013)
Effect of coenzyme Q10 supplementation on heart fail-
ure: a meta-analysis. The American journal of clinical
nutrition 97(2): 268–275.
Garçon G, Leleu B, Zerimech F, et al. (2004) Biologic
markers of oxidative stress and nephrotoxicity as studied
Hormozi et al. 9
11. in biomonitoring of adverse effects of occupational
exposure to lead and cadmium. Journal of Occupational
and Environmental Medicine 46(11): 1180–1186.
Hormozi M, Mirzaei R, Nakhaee A, et al. (2018) The bio-
chemical effects of occupational exposure to lead and
cadmium on markers of oxidative stress and antioxidant
enzymes activity in the blood of glazers in tile industry.
Toxicology and Industrial Health 34(7): 459–467.
Ikematsu H, Nakamura K, Harashima S, et al. (2006)
Safety assessment of coenzyme Q10 (Kaneka Q10) in
healthy subjects: a double-blind, randomized, placebo-
controlled trial. Regulatory Toxicology and Pharmacol-
ogy 44(3): 212–218.
Joseph P (2009) Mechanisms of cadmium carcinogenesis.
Toxicology and Applied Pharmacology 238(3): 272–279.
Kharaeva Z, Gostova E, Luca CD, et al. (2009) Clinical and
biochemical effects of coenzyme Q10, vitamin E, and
selenium supplementation to psoriasis patients. Nutri-
tion 25(3): 295–302.
Lass A and Sohal RS (2000) Effect of coenzyme Q (10) and
alpha-tocopherol content of mitochondria on the pro-
duction of superoxide anion radicals. The FASEB Jour-
nal 14(1): 87–94.
Lee BJ, Huang YC, Chen SJ, et al. (2012) Coenzyme Q10
supplementation reduces oxidative stress and increases
antioxidant enzyme activity in patients with coronary
artery disease. Nutrition 28(3): 250–255.
Lee BJ, Tseng YF, Yen CH, et al. (2013) Effects of coen-
zyme Q10 supplementation (300 mg/day) on antioxida-
tion and anti-inflammation in coronary artery disease
patients during statins therapy: a randomized, placebo-
controlled trial. Nutrition Journal 12(1):142.
Moitra S, Brashier BB and Sahu S (2014) Occupational
cadmium exposure-associated oxidative stress and ery-
throcyte fragility among jewelry workers in India. Amer-
ican Journal of Industrial Medicine 57(9): 1064–1072.
Nzengue Y1, Candéias SM, Sauvaigo S, et al. (2011) The
toxicity redox mechanisms of cadmium alone or
together with copper and zinc homeostasis alteration:
Its redox biomarkers. Journal of Trace Elements in Med-
icine and Biology 25(3): 171–180.
Ognjanović BI, Marković SD, Ethordević NZ, et al. (2010)
Cadmium-induced lipid peroxidation and changes in
antioxidant defense system in the rat testes: Protective
role of coenzyme Q10 and vitamin E. Reproductive Tox-
icology 29(2): 191–197.
Ognjanović BI, Marković SD, Pavlović SZ, et al. (2006)
Combined effects of coenzyme Q10 and Vitamin E in
cadmium induced alterations of antioxidant defense sys-
tem in the rat heart. Environmental Toxicology and
Pharmacology 22(2): 219–224.
Ognjanović BI, Pavlović SZ, Maletić SD, et al. (2003)
Protective influence of vitamin E on antioxidant defense
system in the blood of rats treated with cadmium.
Physiological Research 52(5): 563–570.
Ogunrinola OO, Wusu DA, Fajana OO, et al. (2016) Effect
of low level cadmium exposure on superoxide dismutase
activity in rat. Tropical Journal of Pharmaceutical
Research 15: 115–119.
Oyinloye BE, Ajiboye BO, Ojo OA, et al. (2016) Ameli-
orative potential of Aframomum melegueta extract in
cadmium-induced hepatic damage and oxidative stress
in male Wistar rats. Journal of Applied Pharmaceutical
Sciences 6: 094–099.
Patra RC, Swarup D and Senapati SK (1999) Effects of
cadmium on lipid peroxides and superoxide dismutase
in hepatic, renal and testicular tissue of rats. Veterinary
and Human Toxicology 41(2): 65–67.
Paunović MG, Matić MM, Ognjanović BI, et al. (2017)
Antioxidative and haematoprotective activity of coen-
zyme Q10 and vitamin E against cadmium-induced oxi-
dative stress in Wistar rats. Toxicol Ind Health. 33(10):
746–756.
Rodrı́guez-Carrizalez AD, Castellanos-González JA,
Martı́nez-Romero EC, et al. (2016) The effect of ubiqui-
none and combined antioxidant therapy on oxidative
stress markers in non-proliferative diabetic retinopathy:
A phase IIa, randomized, double-blind, and placebo-
controlled study. Redox Report 21(4): 155–163.
Rosenfeldt FL, Haas SJ, Krum H, et al. (2007) Coenzyme
Q10 in the treatment of hypertension: a meta-analysis of
the clinical trials. Journal of Human Hypertension
21(4): 297–306.
Sciskalska M, Zalewska M, Grzelak A, et al. (2014) The
influence of the occupational exposure to heavy metals
and tobacco smoke on the selected oxidative stress mar-
kers in smelters. Biological Trace Element Research
159(1–3): 59–68.
Seet RC, Lim EC, Tan JJ, et al. (2014) Effects of high-dose
coenzyme Q10 on biomarkers of oxidative damage and
clinical outcomes in Parkinson disease. Antioxidant
Redox Signaling 21(2): 211–217.
Shouroki FK, Shahtaheri SJ, Golbabaei F, et al. (2015)
Measurement of urinary cadmium in glazers using solid
phase extraction followed by inductively coupled
plasma atomic emission spectroscopy. International
Journal of Occupational Hygiene 4(2):11–16.
Shults CW, Flint Beal M, Song D, et al. (2004) Pilot
trial of high dosages of coenzyme Q10 in patients
with Parkinson’s disease. Experimental neurology
188(2): 491–494.
10 Toxicology and Industrial Health XX(X)
12. Somayajulu M, McCarthy S, Hung M, et al. (2005) Role of
mitochondria in neuronal cell death induced by oxida-
tive stress; neuroprotection by Coenzyme Q10. Neuro-
biology of Disease 18(3): 618–627.
Spindler M, Beal MF and Henchcliffe C (2009) Coenzyme
Q10 effects in neurodegenerative disease. Neuropsy-
chiatric Disease and Treatment 5: 597–610.
Stohs SJ and Bagchi D (1995) Oxidative mechanisms in the
toxicity of metal ions. Free Radical Biology and Med-
icine 18(2): 321–336.
Storch A, Jost WH, Vieregge P, et al. (2007) German coen-
zyme Q(10) Study Group. Randomized, double blind,
placebo-controlled trial on symptomatic effects of coen-
zyme Q (10) in Parkinson disease. Archives of Neurol-
ogy 64(7): 938–944.
Tandon SK, Singh S, Prasad S, et al. (2003) Reversal of
cadmium induced oxidative stress by chelating agent,
antioxidant or their combination in rat. Toxicology Let-
ters 145(3): 211–217.
Thompson J and Bannigan J (2008) Cadmium: toxic effects
on the reproductive system and the embryo. Reproduc-
tive Toxicology 25(3): 304–315.
Tiano L, Padella L, Santoro L, et al. (2012) Prolonged
coenzyme Q10 treatment in Down syndrome patients:
effect on DNA oxidation. Neurobiology of Aging 33(3):
626 e621–626 e628.
Uchiyama M and Mihara M (1978) Determination of mal-
ondialdehyde precursor in tissues by thiobarbituric acid
test. Analytical Biochemistry 86(1): 271–278.
Valko M, Morris H and Cronin MT (2005) Metals, toxicity
and oxidative stress. Current Medical Chemistry 12(10):
1161–1208.
Waisberg M, Joseph P, Hale B, et al. (2003) Molecular and
cellular mechanisms of cadmium carcinogenesis: a
review. Toxicology 192(2-3): 95–117.
Wang G and Fowler BA (2008) Roles of biomarkers in
evaluating interactions among mixtures of lead, cad-
mium and arsenic. Toxicology and Applied Pharmacol-
ogy 233(1): 92–99.
Young JM1, Florkowski CM, Molyneux SL, et al. (2012) A
randomized, double-blind, placebo-controlled crossover
study of coenzyme Q10 therapy in hypertensive patients
with the metabolic syndrome. American Journal of
Hypertension 25(2): 261–270.
Hormozi et al. 11