
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Haemostasis and Bleeding Disorders
Similar to Haemostasis and Bleeding Disorders (20)
Recently uploaded
Recently uploaded (20)
Haemostasis and Bleeding Disorders
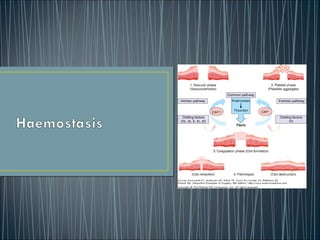
- 2. • Haemostasis is the normal physiological response to prevent significant blood loss following vascular injury • Cellular and molecular mechanisms interact to seal damaged blood vessels with localized clot formation to prevent excessive blood loss • Haemostasis consists of -Primary haemostasis with vascular contraction and platelet formation. -Clotting of the plasma (secondary haemostasis)- Involving interaction between numerous factors and inhibitors -Fibrinolysis- Process for removing the clot once blood vessel’s integrity has been restored.
- 3. • Under normal circumstances blood components pass unhindered through the circulatory system • The vascular barrier provides a non- thrombotic surface due to the production of platelet inhibitors • In contrast, the subendothelial layer is highly thrombogenic- contains collagen, von Willebrand factor (VWF) and other proteins that are involved in platelet adhesion • When the vascular endothelium is disrupted, VWF is released, collagen is exposed and tissue factor (TF) is expressed on the surface of endothelial cells. • The vascular endothelium switches to a prothrombotic state and 1° and 2° haemostasis ensues.
- 4. • Plays a pivotal role in primary haemostasis • Alongside the vessel wall and adhesive proteins, forms the initial ‘platelet plug’ • Activated platelets express phospholipids which promote localised coagulation and the generation of thrombin and fibrin
- 5. • Ligand engagement of G1b/V/IX by VWF/collagen in damaged blood vessels activate platelets • Activated plates changes from discoid (2um) to irregular shape with pseudopods, releasing its granular content (FV, FVIII, Ca, 5- HT, fibrinogen, ADP and thromboxane). • Platelet activation triggers conformational changes in GPIIb/IIIa from inactive state to active state • Fibrinogen and VWF function as bridges between GPIIb/IIIa on neighbouring activated platelets • Activated platelets provide a phospholipid domain, which becomes a catalytic centre for secondary haemostasis.
- 6. • Platelet’s integrin membrane glycoprotein IIb/IIIa increases its affinity to bind fibrinogen. • Fibrinogen crosslinks with glycoprotein IIa/IIIa supporting the aggregation of adjacent platelets.
- 8. • Results in the conversion of thrombin to fibrin, strengthening the aggregated platelets (2°haemostasis) • Damaged blood vessels expressing Tissue Factor [TF] activates coagulation • TF binds to circulating VIIa, forming the ‘Extrinsic tenase’ • In the presence of factor V, converts factor IX IXa and factor XXa • FXa then binds to prothrombin and generates a small amount of fibrin. • Thrombin generation through this reaction is not robust and can be effectively terminated by TF pathway inhibitor
- 9. • Since the amount of thrombin is insufficient to convert fibrinogen to fibrin, numerous positive feedback loops exists • Thrombin generated in the initiation phase further activates FV and VIII, which serves as cofactors in its propagation
- 10. • Continuous thrombin generation is ensured by the action of two complexes: FVIIIa complexed to FIXa (intrinsic tenase), and FVa to Xa (prothrombinase). • This occurs on the surface of platelets and leads to the appropriate localization formation of greater amounts of thrombin.
- 11. The thrombin generated results in the formation of fibrin and activation of factor XIII (fibrin stabilizing factor). FXIII covalent links soluble fibrin monomers to form a stable polymer and provides strength and stability to the fibrin incorporated into the platelet plug.
- 12. • Coagulation is regulated and localized by several anticoagulant mechanisms. • Most important includes anti-thrombin, which inhibits thrombin, and factors IXa, Xa, XIa and XIIa. • Others include TF Pathway inhibitor which inhibits the TF-VIIa complex and thrombin • Activated Protein C, which binds to thrombomodulin and cleaves FVa and FVIIIa.
- 13. • Fibrinolysis is activated at the same time that the coagulation system but operates more slowly and is important for the regulation of haemostasis. • In the presence of fibrin, tissue plasminogen activator (tPA) cleaves plasminogen, producing plasmin which proteolyzes fibrin. • Result in the protein fragment D-dimer, a fibrin degradation product which is a useful marker of fibrinolysis.
- 14. Haemophilia A and B • Haemphilia A and B and the two most common forms of severe inherited bleeding disease. • Both conditions are X-linked recessive • Majority affected individuals are males • 20% of female carriers of haemophilia can also express a mild bleeding tendency (variation pattern of X inactivation) • Diagnosis made through a combination of clinical and laboratory features. • ~60% of cases will have a family history of the condition
- 15. Haemophilia A and B • Clinical manifestations are very similar for factor VIII deficiency (haemophilia A), and factor IX deficiency (haemophilia B) • Severe disease (factor levels <1%) results in frequent episodes of spontaneous musculoskeletal bleeding • Moderate severe disease (factor levels 1-5%) usually do not manifest spontaneous bleeding • Mild haemophilia (factor levels 5-40%) only bleed on provocation • Current treatment involves various forms of protein replacement therapy
- 16. Haemophilia A and B • Schematic showing the intrinsic and extrinsic pathways of the coagulation cascade leading to fibrin formation. A deficiency or dysfunction of coagulation factorVIII orfactorIXcompromises the activation of factorX, the ensuing reactions are inefficient and haemophilia results.
- 17. Von Willebrands Disease • Most common inherited bleeding disorder of humans • Prevalence symptomatic subjects of ~1 in 1000 • Females outnumber males by 2:1 presumably due to manifesting excessive mucocutaneous bleeding at the time on menses and childbirth • 3 types- Type 1 disease is a quantitative deficiency of functionally normal VWF (~65% of VWD cases) Type 2 VWD represents a group of qualitative VWF variants (types 2A, 2B, 2M and 2N) comprising approximately 30% of VWD Type 3 VWD is the virtual absence of VWF (~1 in 1 million of the population )
- 19. Diagnosis of VWD • Diagnosis requires consideration of 3 components- personal history of excessive mucocutaneous bleeding, lab. test consistent with VWD, and a family history of VWD. • Many cases of Type 1 and some type 2 cases can be treated with desmopressin • Remaining cases require transfusion with plasma deprived VWF-FVIII concentrates.
- 21. Haemostasis in LiverImpairment • Liver is involved in the synthesis of most clotting factor proteins • In liver impairment, clotting factor proteins are reduced with the exception of FVIII. • Decreased capacity to clear activated clotting factor-inhibitor complexes. • Liver failure also result in reduced platelet count and function. • These defects are counterbalanced by a concomitant defect in anticoagulant and pro-fibrinolytic factors. • Decreased in platelet function is counterbalanced by elevated levels of Von Willebrand factor. • This rebalance is represented by limited bleeding during surgery. • Coagulopathy in patients with critical liver dysfunction is complex and quickly decompensate to bleeding as well and thrombosis.