4. Targeted cancer
therapies
Dr. Pooja Vaidya
(Second year Resident)
Guide:
Dr. Sandhya Kamat
Professor
Dept. of Pharmacology & Therapeutics
25-08-2016 4
5. “Targeted cancer therapies are drugs that
interfere with specific molecular
structures implicated in tumor growth
and progression”
25-08-2016 5
9. Monoclonal antibodies
• Block cell surface receptors
• Can carry toxins and
radionuclides to the cells of
interest thereby enhancing
their cytotoxic effects
• Specific for a single
receptor
• Long plasma half life
• Intermittent administration
Small molecules
• May also exert effect by
entering cells and
inhibiting enzymatic
functions
• May inhibit multiple
enzymatic sites
• Half life is 12 – 24 hours
• Daily administration
25-08-2016 9
10. 518 Protein kinases
91 Protein tyrosine kinases
(PTKs)
Serine/threonine kinases &
others
Eg: TGF-β, RAF, ERK, MEK,
Cyclin dependent kinases
59 Receptor PTKs
32 Non receptor PTKs
Eg. ABL, JAK
Trans membrane glycoproteins
Eg: ErB family of receptors,
PDGFR
Targeted cancer therapies
25-08-2016 10
11. Imatinib mesylate
First molecularly targeted protein kinase inhibitor to
receive FDA approval in 2003
Targets the BCR-ABL tyrosine kinase in a closed or inactive
configuration
25-08-2016 11
13. To overcome the resistance to Imatinib
binds to multiple states of
kinase including active
conformation
targets both ABL & SRC
kinases
active against almost all of
the clinically relevant
mutants, the exception
being the T315I mutant
more potent and less toxic
than Imatinib
Target the active
kinase conformation
Target substrate binding
site
ON012380
Dasatinib & Nilotinib
Effective against all
mutants including T315I
Synergises well with
Imatinib
25-08-2016 13
14. Imatinib, Dasatinib & Nilotinib
Additional therapeutic benefits in,
GIST ( kit mutation positive)
Chronic myelomonocytic leukemia
Hypereosinophilia syndrome
Dermatofibrosarcoma protuberans
Dose: Imatinib: 250 – 750mg/day
Dasatinib: 100 mg daily (chronic CML)
70 mg BD (advanced CML)
Nilotinib: 400 mg twice daily
Bioavailability of Nilotinib increases in the presence of food
ADR: Fluid retention & hepatotoxicity
Dasatinib may cause pleural effusions
Nilotinib may prolong the QT interval25-08-2016 14
17. Gefitinib and Erlotinib
Responsive tumors have specific activating mutations in the
EGFR kinase domain which convert EGFR into a strongly
oncogenic form that can be an essential tumor survival factor
Act by targeting tumor survival factors
Standard dose of Gefitinib is 250 mg daily
In 2003, Gefitinib was approved for the third-line treatment of
patients with NSCLC, but, two large trials have failed to
demonstrate significant survival benefit
But, Gefitinib continues to be widely used outside the U.S
Both metabolized by CYP3A425-08-2016 17
18. Erlotinib is approved for,
Second-line treatment of patients with locally advanced or
metastatic NSCLC (150 mg daily )
First-line treatment of patients with locally advanced,
unresectable, or metastatic pancreatic cancer in
combination with gemcitabine (100 mg daily )
Food increases bioavailability of Erlotinib to 100%,
so should not be taken with food
Concurrent PPI decreases the bioavailability of Erlotinib by
50%
ADR: Diarrhoea , pustular/papular rash
Asymptomatic increases in liver transaminases
Interstitial lung disease in <2% cases but may have a fatal
outcome.
Gefitinib and Erlotinib
25-08-2016 18
21. Cetuximab is FDA approved for,
locally or regionally advanced HNSCC
EGFR-positive metastatic colorectal cancer
Single loading dose of 400 mg/m2 I.V. followed by weekly doses
of 250 mg/m2
Panitumumab FDA approved as,
First-line therapy in combination with FOLFOX in patients
with wild-type KRAS mCRC
Based on improved OS of 4.4 months in phase 3 PRIME study
Dose: 6 mg/kg intravenously given once every 2 weeks
ADR: Acne form rash, headache, and diarrhoea
Cardiopulmonary arrest, interstitial lung disease, and
hypomagnesemia
Cetuximab & Panitumumab
25-08-2016 21
22. ErbB2 or HER 2/neu inhibitors
First mab approved for solid
tumor
Currently approved for
HER2/neu-overexpressing
metastatic breast cancer, in
combination with paclitaxel
as initial treatment or as
monotherapy following
chemotherapy relapse
Most serious toxicity is
cardiac failure
Trastuzumab
Lapatinib
Blocks both ErbB1 and ErbB2
Inhibits the truncated form of
HER2 that lacks the
trastuzumab binding domain
FDA-approved for HER2-
amplified, trastuzumab-
refractory breast cancer, with
capecitabine
Crosses the BBB
ADR: Diarrhoea, rash25-08-2016 22
23. Targeting angiogenesis
Judah Folkman: opened the field of anti-angiogenesis therapy
Jain: proposed an additional mechanism,
Capillary permeability and tumor interstitial pressure
Inhibition of blood flow and drug delivery within the tumor
Targeting primary angiogenic factor would normalize interstitial
pressure & improve blood flow
Enhance the ability of chemotherapeutic agents to reach the tumor
25-08-2016 23
25. Bevacizumab
FDA approved for,
mCRC with combination chemotherapy
First-Line Treatment of NSCLC in combination with
carboplatin and paclitaxel
Metastatic RCC in combination with interferon- alpha
As a single agent following prior therapy for GBM
Recurrent, or metastatic cervical cancer in combination
with paclitaxel
Doses vary reflecting the designs of approval directed trials
Plasma t1/2: 4 weeks
ADR: Risk of bleeding, hypertension, proteinuria, arterial
thromboembolic event, GI perforation
25-08-2016 25
26. Sunitinib and Sorafenib
Multi-targeted tyrosine kinase inhibitor
Targets tyrosine kinase domain on the VEGFR-2, FLT3, PDGFR-α,
PDGFR- β , RET, CSF-1R, and c-KIT
Sunitinib approved for treatment of advanced renal-cell
carcinoma and Imatinib resistant GIST
50 mg once a day for 4 weeks followed by 2 weeks off treatment
Metabolized by CYP3A4 and t1/2 is 80 - 110 hours
Sorafenib is the only drug currently approved for treatment of
hepatocellular carcinoma
Also approved in metastatic renal-cell cancer
400 mg twice daily without treatment breaks
Metabolized by CYP3A4 and t1/2 is 20 - 27 hours
25-08-2016 26
28. PI3K/PKB(Akt) /MTOR inhibitors
FDA approved Temsirolimus and Everolimus for Renal cancer
Dose: Temsirolimus 25 mg/week IV
Everolimus 10 mg/day oral
Administered in the fasting state at least 1 hour before a meal
Also, implicated in,
Hepatocellular cancer
Mantle cell lymphoma
Endometrial cancer
Metabolized by CYP3A4
Toxicity: maculopapular rash, mucositis, anemia, and fatigue
25-08-2016 28
30. Other kinase inhibitors
Drug Target Disease Clinical trial
stage
Other potential indications
Crizotinib
(PF02341066
)
ALK Lung cancer
(EML4-ALK
fusion)
Phase 3 Anaplastic lymphoma,
neuroblastoma,
Inflammatory
myofibroblastic
sarcoma
Vandetanib,
Sorafenib,
Motesanib
RET Thyroid
cancer
Phase 3
Midostaurin
AC220
FLT - 3 FLT mutant
Acute myeloid
leukaemia
Phase 3 FLT mutant ALL
INCB018424
TG101348
JAK-2 Myelofibrosis Phase 3
Phase 2
Polycythemia vera
Essential thrombocytosis
Axitinib
Tivozanib
Pazopanib
VEGFR Renal cancer Phase 3 Hepatocellular carcinoma
25-08-2016 30
31. Targeting nuclear factors: Bortezomib
NF-κB: tumor survival factor in hypoxic environment and
during chemotherapy
Blocks ubiquitin proteasomal protein degradation pathway,
thereby preventing the transcriptional activity of NF-κB and
down regulating survival responses
FDA approved
as initial therapy for Multiple Myeloma and as therapy for MM
after relapse from other drugs
for relapsed or refractory mantle cell lymphoma
Dose: 1.3 mg/m2 I.V. bolus on days 1, 4, 8, and 11 of every 21-
day cycle with a 10-day rest period per cycle
Plasma t1/2: 5.5 hours
Toxicity: Pancytopenia, fatigue, peripheral neuropathy,
hypotension
25-08-2016 31
32. Targeted Anticancer Therapies Using Antibodies
Monoclonal antibodies have become a major strategy in
clinical oncology
Specifically bind to primary and metastatic cancer cells
with high affinity
Antitumor effects by
complement mediated cytolysis and antibody-dependent
cell-mediated cytotoxicity (naked antibodies)
By the focused delivery of radiation or cellular toxins
(conjugated antibodies)
25-08-2016 32
34. Generic
name
Target; Format Indication EU
approval
US
approval
Rituximab CD20; Chimeric
IgG1
NHL 1998 1997
Trastuzumab HER2; Humanized
IgG1
Breast cancer 2000 1998
Gemtuzumab
ozogamicin
CD33; Humanized
IgG4
AML
NA
2000 ##
Alemtuzumab CD52; Humanized
IgG1
CLL
Multiple
sclerosis
2001 ##
2013
2001 ##
2014
Ibritumumab
tiuxetan
CD20; Murine IgG1 NHL 2004 2002
Tositumomab
- I131
CD20; Murine
IgG2a
NHL NA 2003 ##
Approved Monoclonal antibodies
25-08-2016 34
35. Approved Monoclonal antibodies
Generic
name
Target; Format Indication EU
approval
US
approval
Cetuximab EGFR; Chimeric IgG1 Colorectal
cancer
2004 2004
Bevacizumab VEGF; Humanized IgG1 Colorectal
cancer
2005 2004
Panitumumab EGFR; Human IgG2 Colorectal
cancer
2007 2006
Ofatumumab CD20; Human IgG1 CLL 2010 2009
Ipilimumab CTLA-4; Human IgG1 Metastatic
melanoma
2011 2011
Brentuximab
vedotin
CD30; Chimeric IgG1;
Immunoconjugate
Hodgkin
lymphoma
2012 2011
25-08-2016 35
36. Approved Monoclonal antibodies
Generic name Target; Format Indication EU
approval
US
approval
Pertuzumab HER2; humanized IgG1 Breast
Cancer
2013 2012
Ado-
trastuzumab
emtansine
HER2; humanized IgG1;
Immunoconjugate
Breast
cancer
2013 2013
Obinutuzumab CD20; Humanized IgG1;
Glycoengineered
CLL 2014 2013
25-08-2016 36
37. Monoclonal antibodies in review
Generic name Target; Format Indication EU
approval
US
approval
Ramucirumab VEGFR2; Human
IgG1
Gastric
cancer
Pending 2014
Pembrolizumab PD1; Humanized
IgG4
Melanoma In review 2014
Nivolumab PD1; Human IgG4 Melanoma In review 2014
Blinatumomab CD19, CD3 ALL In review 2014
Necitumumab EGFR; Human IgG1 NSCLC In review In review
25-08-2016 37
38. Target and drug evaluation
Target validation
Appropriate preclinical models
Desired target is known to be expressed
Target is important for cell/ tumour survival
In - vitro screening In - vivo models
a cancer cell line /genetically
engineered cell line
Lead compound tested for
target inhibition
Confirmed by biochemical
studies
Xenograft model in
immunocompromised
mice
Orthotopic grafts:
metastatic cancer
Transgenic models25-08-2016 38
39. Combination therapies
To target the cancer stem cells
Eg: Interferon + Imatinib for CML
To target several different pathways that affect tumor
growth
Eg: Erlotinib and Bevacizumab in RCC
Targeted inhibition can sensitize cancers to
chemotherapy and radiotherapy
Eg: Trastuzumab + chemotherapy in breast cancer
25-08-2016 39
40. 25-08-2016 40
Take home message…
Molecularly targeted therapy is a new way of approaching cancer
treatment
Involves rational selection of drugs which target specific
processes in cancer cells that make them different from normal
cells
A number of targeted therapies are currently available and many
others are in development
Targeted therapies are frequently effective but there are side
effects to the treatments, and development of resistance
Targeted therapies are increasingly being used in combination
with other targeted therapies or with other treatment modalities
41. The Future Is Now:
Pharmacogenomics and Personalized Medicine
Personalized treatment using genomic or proteomic
techniques
To determine the most susceptible molecular targets in a
specific patient
To predict the likelihood that a patient will
respond to a specific chemotherapy regimen
To predict the risk of toxic side effects
25-08-2016 41
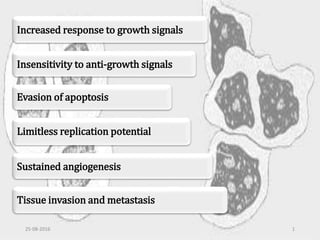
What Makes Cells Cancerous?...
All cancers acquire the same six hallmark capabilities…
In some cases, a particular mutation may confer several capabilities (e.g., P53, the guardian of the genome may undergo mutation and cause resistance to apoptosis), whereas in other cases, multiple mutations may be required to enable a single capability.
Many new anti-cancer drugs recently approved or in late stages of evaluation are designed to block the fundamental mutations that cause specific cancers…like..
Those resulting in aberrant growth factor receptors, defective DNA repair and Apoptosis, Dysregulated intracellular signalling pathways and Tumour angiogenesis.
Now, in case of signalling pathways ….
In normal cells, when one pathway is inhibited, the effect on the cell is minimized by the presence of alternative, redundant pathways.
Whereas, cancer cells are particularly sensitive to inhibition of their overexpressed or hyper activated signaling protein. And Redundancy is reduced in cancer cells, owing to the large number of mutations that these cells sustain.
Thus, cancer cell survival and proliferation depend on a few hyperactive signaling pathways,
an Achilles’ heel that the therapist can attack
Currently …we are shifting from a “black box” approach to specific, targeted therapy for the treatment of cancer
And thus …the importance of targets in cancer treatment…and this forms the premise for TCT.
So, today… i will be talking on Targeted cancer therapies.
Every cell in the body contains 30,000 genes.
Each of these genes makes a different protein and each protein performs a different task. Targeted therapies stop specific proteins from helping cancer survive. When certain specific proteins are blocked, the cancer cells can’t grow and they die.
Thus, TCT are drugs that …..
The main strategies to achieve this ..is by targeting cellular proliferation, …..
The primary tools for inhibiting these targets are either monoclonal antibodies that attack cell surface receptors and antigens, or synthetic small molecules that enter cells and engage critical enzymes..
But, now, the point to be noted is that.. The two classes of drug, when targeted against the same pathway, may have significantly different spectra of antitumor activity. As shown in the figure here,
monoclonal antibodies to the epidermal growth factor receptor (EGFR) are effective in the treatment of head and neck and colon cancers,
while small molecules against the intracellular tyrosine kinase function of the same receptor have a different spectrum of antitumor activity in non–small cell lung cancer..
Now, For the purpose of discussion, I have classified the targeted cancer therapies based on the predominant target on which they act
Structurally and functionally different molecules, may act on the same target and will be described based on the predominant target in my discussion.
The basic difference between these two classes of drugs are..
Small molecules may attack the same targets and pathways as the monoclonals, but may also exert their effect by entering cells and inhibiting enzymatic functions
Recognizing the families of proteins.. involved in the initiation, progression, and spread of cancer enables us to think rationally about which pathways to manipulate in order to suppress the disease. And.. the most popular candidates for targeted therapy are protein kinases.
PKs control the balance between cell cycle progression, cell cycle arrest, and cell death and have been implicated in cancer.
The human genome includes about 518 PKs. 91 of these are protein tyrosine kinases (PTKs), and others include Serine/Threonine kinase and others. Eg: TGF beta kinase, RAF kinase, MEK kinase, ERK kinase etc…
PTK comprise of 59 receptor PTKs (RPTKs) and 32 non receptor PTKs.
RPTKs are trans membrane glycoproteins Eg: ErB family of receptors, PDGF R.
NR PTK’s ..Eg: ABL, JAK
ERK: Extracellular signal – regulated kinase
RAF: Rapidly Accelerated Fibrosarcoma
MEK/MAPK: Mitogen activated protein kinase
ABL: Abl stands for "Abelson", the name of a virus which carries a similar protein.
Imatinib received fast-track approval by the FDA as an ATP-competitive selective inhibitor of bcr-abl
Imatinib bind to a segment of the bcr-abl kinase domain that fixes the enzyme in a closed or non functional state, in which protein is unable to bind ATP, thereby inhibiting the signalling pathway.
One important point to be noted is that Imatinib is an inhibitor of the closed, or inactive, configuration of the kinase.
Also, later it was realized that BCR‐ABL kinase is the major survival element in the leukemic cells in early phase CML. This is not the case for more advanced disease. So,
Only a temporary effect was seen with Imatinib in acute CML, with disease recurrence in a matter of months
Imatinib does not eradicate CML, relapse occurs if treatment is stopped
Therefore, patients are now kept on Imatinib indefinitely, unless resistance emerges
A number of mechanisms of resistance to Imatinib have been characterized, the most common being mutations in the ABL kinase domain.
The mutations lock the enzyme in its open configuration, in which it has access to substrate
Other mechanisms of resistance include amplification of the BCR‐ABL gene, activation of BCR‐ABL independent alternative oncogenic pathways like the SRC signalling pathway.. And other minor mechanisms like presence of multidrug resistant (MDR ) gene which codes for a drug efflux protein.
The realization of resistance lead to development of new targets …
To overcome resistance, new drugs were tested that can bind both active and inactive forms of the kinase and Dasatinib & Nilotinib were developed.
less toxic.. because the active state of enzyme is present only transiently in healthy cells, whereas it is the predominant form of the enzyme in the targeted cancer cells.
Also, being a dual Src‐Abl inhibitor such as Dasatinib provides “combination” therapy in a single formulation.
Now, most current PTK inhibitors, including Imatinib, are ATP competitive inhibitors. But they tend to be poorly selective and target several related kinases.
Another way to overcome resistance is targeting the substrate binding site. Recently, a substrate‐competitive inhibitor of BCR‐ABL, ON012380 has been developed.
T315I mutant wherein Threonine is replaced by isoleucine at 315 position
These Tyrosine kinase inhibitors have efficacy in diseases in which the ABL, kit , or PDGFR have dominant roles in driving the proliferation of the tumor.
Remarkable therapeutic benefits also seen in patients GIST ( kit mutation positive), chronic myelomonocytic leukemia (EVT6-PDGFR translocation), hypereosinophilia
syndrome (FIP1L1-PDGFR), and dermatofibrosarcoma protuberans (constitutive production of the ligand for PDGFR)
Food does not change the pharmacokinetic profile of Imatinib & Dasatinib... but..
All three drugs promote fluid retention, which may lead to dependent edema, and peri-orbital swelling
The EGFR family comprises four members:
EGFR (ErbB1), ErbB2 (Her‐2), and ErbB4 have catalytic activity; ErbB3 is catalytically inactive but retains ligand binding.
Ligand binding to the extracellular domain stimulates the protein tyrosine kinase activity of the intracellular domain which initiates protein-protein interactions that result in stimulation of a variety of signaling pathways
Overexpression and/or abnormal activation of EGFR family members is associated with a wide spectrum of solid tumors, including non‐small cell lung carcinoma, breast cancer, pancreatic cancer, colon cancer, glioblastoma and head and neck cancer
Two separate classes of drugs that target the EGFR pathway have become important agents in the therapy of solid tumors. Small molecules ie. The EGFR tyrosine kinase inhibitors erlotinib and gefitinib bind to the kinase domain and block the enzymatic function of EGFR. The monoclonal antibodies cetuximab and panitumumab bind specifically to the extracellular domain of EGFR.
EGFR is overexpressed in over 80% of NSCLC, so it was hoped that drugs like Gefitinib would have a major impact on treatment of the disease. But these hopes were shattered when only 10% of NSCLC patients responded to Gefitinib in clinical trials in the United States. The frequency of response to Gefitinib was higher among women, non-smokers, and East Asians. Then it was found that the responsive tumours…
New clinical trials are being developed, other ongoing trials are being completed. These will determine the future role of Gefitinib treatment. But, Gefitinib continues to be widely used outside the U.S
Diarrhea and pustular/papular rash occur in ~50% of patients taking gefitinib
Second-line treatment of patients with locally advanced or metastatic NSCLC (based on improvement in overall survival in a large multi-national trial comparing oral Erlotinib, 150 mg daily, to placebo)
First-line treatment of patients with locally advanced, unresectable, or metastatic pancreatic cancer in combination with gemcitabine (based on a double-blinded study of 569 patients which demonstrated a modest 2-week improvement in overall survival in patients who received 100 mg of erlotinib plus gemcitabine, as compared with patients who received gemcitabine alone)
But, Resistance to Gefitinib and Erlotinib arises through several different mechanisms
A secondary mutation in the EGFR gatekeeper residue, T790M, prevents binding of drug to the kinase domain and confers resistance. Irreversible EGFR inhibitors currently are in clinical development to overcome this mechanism.
Amplification of the met oncogene provides an alternative pathway to clinical resistance by activating cell growth signals downstream of EGFR. Such MET -amplified tumors respond in vitro to the simultaneous inhibition of EGFR and MET in combination therapies
Both bind to extracellular domain of EGFR & prevents ligand dependent signalling and receptor dimerization, thereby blocking cell growth and survival signals.
Cetuximab is fda approved for metastatic colorectal cancer, but, numerous trials now have shown that the 40-50% of colorectal tumors carrying mutations in the k-ras oncogene are resistant to the effects of cetuximab. The antibody yields a response rate of 1% in patients with mutant tumors, compared to 12% in k-ras wild-type tumors
mCRC: metastatic colorectal cancer
HNSCC: squamous cell carcinoma of head & neck region
In this case, both monoclonal antibody trastuzumab and small molecules lapatinib have striking antitumor effects in patients with HER2-positive breast cancer, and have become essential therapeutic agents.
Trastuzumab was the first monoclonal antibody to be approved for the treatment of a solid tumor. This humanized Mab binds to the external domain of HER2/neu, thereby preventing receptor kinase activation and downstream signaling and blocks of the angiogenic effects of HER2 signaling.
Currently, it is approved for HER2/neu-overexpressing metastatic breast cancer, in combination with paclitaxel as initial treatment or as monotherapy following chemotherapy relapse. The most serious toxicity of trastuzumab is cardiac failure; reasons for cardio toxicity are poorly understood.
Lapatinib: block both ErbB1 and ErbB2. 2 main advntages of Lapatinib are, It inhibits the truncated form of HER2 that lacks the trastuzumab binding domain, responsible for activity in trastuzumab resistant patients. FDA-approved for HER2-amplified, trastuzumab-refractory breast cancer, in combination with capecitabine.
Being a small molecule, lapatinib crosses the blood-brain barrier more readily than inhibitor antibodies and has produced anecdotal responses in patients with brain metastases
ADR: Diarrhoea, rash, no cardio toxicity noted with its use.
he hypothesized that angiogenesis-is an essential property of cancer. Cancer cells secrete angiogenic factors like VEGF , FGF , TGF- β , PDGF that induce the formation of new blood vessels and guarantee the flow of nutrients to the tumor cells. Multiple tumor types overexpress these angiogenic factors.
Jain has proposed an additional mechanism for the efficacy of angiogenesis inhibitors.
Increased capillary permeability within tumors cause an increase in tumor interstitial pressure. Increased pressure inhibits blood flow, decreases oxygenation, and prevents drug delivery within the tumor. Antibodies directed at the primary angiogenic factor normalize interstitial pressure, improve blood flow.
Enhance the ability of chemotherapeutic agents to reach the tumor
The best studied of the angiogenic factors is VEGF.
VEGF receptor family includes VEGFR1 (FLT1), VEGFR2 (KDR), and VEGFR3 (FLT4). The binding of VEGF to its receptor activates the intracellular VEGFR tyrosine kinase activity and initiates mitogenic and anti-apoptotic signaling pathways.
The cognate interaction between VEGF and its receptor creates several opportunities for pharmacological inhibition of this pathway.
Bevacizumab humanized antibody directed against VEGF-A, is the first FDA-approved molecule that specifically targeted angiogenesis.
Small molecules ( sorafenib, and sunitinib) that inhibit the kinase function of VEGFR-2 have been approved for clinical use
Also, an investigational drug Aflibercept , is a recombinant fusion protein that combines VGFR-1 & VGFR-2 binding domains with Fc region of human IgG1 antibody to sequester VEGF-A, therby acting as acts as VEGF Trap… available with the brand name..Zaltrap !!
Recently in 2014, US FDA approved Bevacizumab for the treatment of persistent, recurrent, or metastatic cervical cancer in combination with paclitaxel.
The differing doses of bevacizumab reflect the varying designs of approval-directed trials.
The most dreaded vascular toxicity of anti-angiogenic agents is an arterial thromboembolic event (i.e., stroke or myocardial infarction. A meta-analysis found that the rate of arterial thromboembolic events in patients receiving bevacizumab-containing regimens reached 3.8% compared to the control rate of 1.7%
Sunitinib is approved for treatment of advanced renal-cell carcinoma and GIST that have developed resistance to imatinib as a consequence of c-KIT mutations
CSF-1R: Colony stimulating factor -1 receptor
The phosphatidyl inositol (PI-3) kinase pathway is central to intracellular signalling. PI3-kinase,a type of receptor tyrosine kinase, is activated by many growth factor receptors and leads to the formation of the intracellular messenger PIP3. And the downstream effectors, the mechanistic target of rapamycin (mTOR) modulates cell growth, metabolism, and apoptosis.
The tumor suppressor PTEN dephosphorylates PI3K.
Activating mutations and amplification of genes in the receptor-PI3K pathway, and loss of function alterations in PTEN, occur frequently in cancer cells, with the result that PI3K signaling is exaggerated and cells lose growth control and exhibit enhanced survival (decreased apoptosis).
Rapamycins & its congeners exert anti-tumour action from their binding to FKBP12 and inhibition of mTOR and thus inhibit cell-cycle progression, angiogenesis, and promote apoptosis.
This pathway is activated in human tumours by several mechanisms.. including binding of ligand to receptor tyrosine kinases or mutations in RAS, BRAF and MEK---This leads to activation of ERK which regulates gene transcription thereby promoting cell cycle progression and tumour survival.
Also, this pathway has a classical negative feedback loop and in case of tumours with a mutant BRAF, the pathway output is enhanced due to impaired upstream feedback regulation.
So, drugs against these new targets are currently in clinical development…
PD325901 and AZD6244 target MEK. The clinical development of PD325901 was discontinued due to safety concerns of ocular & neurological toxicities. AZD6244 is currently in phase 2 trials in patients with BRAF mutant melanoma.
Also, Phase 1 trial with a third MEK inhibitor ,GSK1 120212, have reported a high response rate of 40% in BRAF-mutant melanoma patients.
In 2009 -2010, dramatic clinical response was observed with novel selective BRAF inhibitor PLX4032. Currently it is in phase 3 clinical trial.
Also, impressive responses were observed in Phase 1 trial with BRAF mutant melanoma patients with more potent BRAF inhibitor GSK2118436
Other unapproved kinase inhiitors with a clear evidence of clinical activity include,
1. ALK: Anaplastic lymphoma kinase
2. Drugs specifically designed to target RET are not available, but 3 drugs i.e. Vandetanib, Sorafenib and Motesanib having activity against RET are under evaluation in phase 3 clinical trials in thyroid cancer patients. Of these, Vandetanib has recently reported improved progression-free survival
3. In approximately 30% of cases of AML, a flt-3 gene mutation creates abnormal FLT-3 receptor that promotes the growth and survival of the leukemic cells. Midostaurin is being evaluated in phase 3 trials in new cases of AML in combination with induction chemotherapy. AC 220 is the next generation flt-3 inhibitor with a impressive single agent activity in relapsed cases of flt mutant AML.
4. The discovery of JAK-2 mutations in polycythaemia, essential thrombocytosis and myelofibrosis provided a unifying understanding of myeloproliferative disorders and 2 compounds INCB018424 and TG101348 are in phase 3 and phase 2 studies respectively in myelofibrosis
NF- B is highly expressed in many human tumors, including MM, and may be a key factor in tumor cell survival in a hypoxic environment and during chemotherapy
Initial MAbs used were murine in origin and patients developed human antimouse antibody responses against the therapeutic agents. Thereafter using genetic engineering technologies, chimeric, humanized and fully human Mab’s are developed.
Therapeutic monoclonal antibodies are typically of the IgG class containing two heavy and two light chains.
Initial MAbs used were murine in origin and patients developed human antimouse antibody responses against the therapeutic agents. Thereafter Advance in antibody therapeutics began in the early 1980s when using genetic engineering technologies, chimeric, humanized and fully human Mab’s are developed.
Accordingly these are referred to with the suffix.. respectively
Currently , the U.S. FDA has approved 16 antibodies for the treatment of cancer and many more are under evaluation in late-stage clinical trials.
Approved in 1997, rituximab is arguably the most commercially successful anticancer drug. Targeting the CD20 surface receptor common
to many B cell non-Hodgkin lymphoma subtypes, rituximab is a chimeric monoclonal IgG1 antibody that induces apoptosis, antibody dependent cell cytotoxicity, and complement mediated cytotoxicity.
Thereafter, Trastuzumab was approved..
The approval of gemtuzumab marked the first introduction of a plant toxin conjugated antibody. The drug received accelerated approval for patients with AML but later was withdrawn from market as drug failed to show clinical benefit in patients enrolled in trials and there were concerns regarding serious liver condition seen in post marketing surveillance
Alemtuzumab, which targets CD52 was originally approved for treatment of patients with CLL ..but the company voluntarily withdrew the drug from the markets in 2012 to prevent off label use to treat multiple sclerosis and to prepare for a relaunch the drug with a different dosage and at a higher price ..which then received approval in 2014.
In 2002 Ibritumomab tiuxetan became the first radioconjugated therapeutic antibody approved by the FDA in patients with NHL. Therafter, anti-CD20 murine monoclonal antibody, I131 radiolabeled-Tositumomab was approved in 2003 for the treatment of non-Hodgkin lymphoma. But, recently in 2014 drug was withdrawn due to the decline in usage !!
Then Cetuximab, Bevacizumab and Panitumumab were approved for treatment of colorectal cancer
Then in 2009, a fully human anti-CD20 antibody Ofatumumab was approved for treatment of patients with CLL. Additional humanized anti-CD20 antibodies (veltuzumab and ocrelizumab) are under development.
Cytotoxic T-lymphocytes can recognize and destroy cancer cells. However, there is a inhibitory mechanism that interrupts this destruction. Ipilimumab turns off this inhibitory mechanism by targeting and allows t-lymphocytes to continue to destroy the cancer cells. This human antibody was approved for patients with Metastatic melanoma.
In 2011, another Immunoconjugate antibody, Brentuximab vedotin was approved for Hodgkin’s lymphoma. This is the most advanced and promising anti-CD30 construct so far, consisting of antibody and synthetic antimitotic agent.
Recently, in 2012... Pertuzumab, humanized IgG1 antibody against HER2 & Immunoconjugate antibody Adotrastuzumab received approval for Breast cancer.
Obinutuzumab, a second generation Glycoengineered anti-CD 20 antibody, is approved for CLL recently in 2014. Glycoengineering is the term used to refer to manipulation of sugar molecules to improve the binding of monoclonal antibodies with immune effector cells
Coming to Mab’s which are in review …
In 2014, USFDA approved Ramucirumab for gastric cancer, Pembrolizumab for Melanoma, Binatumumab for ALL and Nivolumab for melanoma. The approval of these in the European countries in pending .
Blinatumomab enables a patient's T cells to recognize malignant B cells. A molecule of the drug combines two binding sites: a CD3site for T cells and a CD19 site for the target B cells and direct the human immune system to act against tumor cells.
A human IgG1 antibody against EGFR, Necitumumab is in review for patients with NSCLC
PD1: Programmed cell death protein 1 OR CD279
The shift from cytotoxic chemotherapy to targeted signal transduction therapy necessitates a shift in preclinical drug assessment strategies.
Target validation is a critical step toward verifying a proposed mechanism of action. i.e. The drug should be tested on appropriate preclinical models in which the desired target is known to be expressed and to be important for cell/tumor survival.
When designing targeted therapy, we have a specific molecular target in mind. Such projects often begin with an in vitro screen for inhibitors of that target. This will employ a cancer cell line or a genetically engineered cell line in which the target is known to be strongly activated because of either mutation or overexpression (or both) and the Lead Compound is then tested and inhibition of the target is confirmed by biochemical studies.
Good in vitro models would simplify screening for cancer drugs, but, these models does not consider the role of the surrounding stromal tissue, interstitial space, blood vessels, or the immune system in tumor development.
The, coming to In-vivo models.. xenograft models in immunocompromised mice are useful for preliminary pharmacological characterization.
xenografts are often subcutaneous, in which case growth of a solid tumor can be easily assessed. Injecting these types of xenografts does not require any particular surgical skills.
When it is important to imitate the natural environment of the tumor, such as when studying angiogenic factors, an orthotopic (i.e., to the same tissue) xenograft may be preferred. Orthotopic grafts are better models for metastatic cancer.
Transgenic Models are expensive and difficult to establish but have an advantage that they can be generated in immunocompetent mice
Both hematopoietic and solid tumors include a population of self‐renewing “cancer stem cells”. Thus, even if the bulk of a tumor is eradicated, the cancer stem cells may be capable of regenerating the tumor. In vitro studies show that CML stem cells are more sensitive to interferon whereas the differentiated cells are more sensitive to Imatinib. The combination is effectively used.
Erlotinib and Bevacizumab: In a clinical trial in 59 patients with metastatic RCC, tumor load was reduced by at least 50% in 21% of patients, and the disease stabilized in a further 66%. At 18 months, 60%of patients were still alive.
Targeted inhibition can sensitize cancers to chemotherapy and radiotherapy such that doses can be reduced and toxic side effects minimized.
About a quarter of breast cancers overexpress ErbB2. These tumors are resistant to hormone therapy and, until recently, carried a poorer prognosis. Inhibition of ErbB2 by small molecules or by the monoclonal antibody trastuzumab is synergistic with certain forms of chemotherapy and shown to improve prognosis. Also, treatment by chemotherapy plus Herceptin was twice as effective in preventing the recurrence.
Furthermore, combining therapies is the most effective method to reduce the emergence of resistance
We definitely will be hearing much more about targeted therapies for cancer in the future
Targeted therapy in oncology has been a major stimulus for the evolving field of pharmacogenomics.
“Personalized treatment” using genomic or proteomic techniques to determine which are the most susceptible molecular targets in a specific patient, is still a futuristic idea, but ..no longer a wild science fiction fantasy.
It would be possible to predict the likelihood that a patient will respond to a specific chemotherapy regimen and to predict the risk of toxic side effects
During the next several years, the field of oncology drug development will see numerous products pass through the approval process and enter the market accompanied by diagnostic tests designed to “personalize” their use, dosage, route of administration, and length of treatment for each patient, one at a time.
Only time will tell whether this new approach to anticancer pharmaceuticals will yield breakthrough results, reducing morbidity and mortality and improving outcomes for all who will be afflicted with the disease