
Recommended
More Related Content
Similar to Lecture on Orbit Cellulitis For 4th Year MBBS Undergraduate Students By Prof. Dr. Hussain Ahmad Khaqan
Similar to Lecture on Orbit Cellulitis For 4th Year MBBS Undergraduate Students By Prof. Dr. Hussain Ahmad Khaqan (20)
More from DrHussainAhmadKhaqan
More from DrHussainAhmadKhaqan (20)
Recently uploaded
Recently uploaded (20)
Lecture on Orbit Cellulitis For 4th Year MBBS Undergraduate Students By Prof. Dr. Hussain Ahmad Khaqan
- 1. Orbital Cellulitis Prof. Dr. Hussain Ahmad Khaqan MD FRCS(Glasgow) FCPS(Ophth.) FCPS(Vitreo Retina) MHPE (KMU) CICO(UK) CMT(UOL) Fellowship in Medical Retina (LMU, Munich) Fellowship in Vitreo Retinal Surgery (LMU, Munich) Consultant Ophthalmologist & Retinal Surgeon Professor of Ophthalmology Lahore General Hospital, Lahore Ameer Ud Din Medical College, Lahore Post Graduate Medical Institute, Lahore Shaukat Khanum Memorial Cancer Hospital & Research Centre ,Lahore
- 2. DEFINITION • Inflammation or infection of the orbital contents.
- 3. SYMPTOMS • Fever, malaise • Blurred vision • Double vision • Reduced ocular motility • Red eye • Eyelid and/or periorbital swelling • Nasal congestion/discharge, sinus headache/pressure/congestion, tooth pain, infra- and/or supraorbital pain, or hypoesthesia.
- 4. SIGNS CONTINUE.. • Inflamed lids (swollen, red, tender, warm) ± chemosis, proptosis, painful restricted eye movements, , lagophthalmos • purulent discharge.
- 5. SIGNS • Decreased periorbital sensation • Optic nerve dysfunction (VA, Colour vision, RAPD). • Retinal venous congestion • Optic disc edema
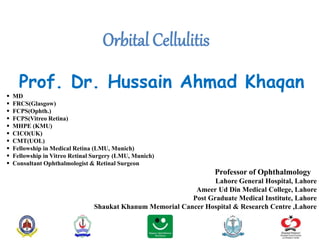
- 6. INVESTIGATION CONTIUNE.. • Imaging: CT/MRI scan of the orbits and paranasal sinuses (axial, coronal, and parasagittal views, with contrast if possible) to confirm the diagnosis and to rule out a retained foreign body, orbital or sub periosteal abscess (SPA), paranasal sinus disease, cavernous sinus thrombosis, or intracranial extension.
- 7. Figure: CT orbit (A) axial view (B) Coronal view
- 8. CAUSES • Direct extension from a paranasal sinus infection (especially ethmoiditis), focal periorbital infection (e.g. , infected hordeolum, dacryoadenitis, dacryocystitis, panophthalmitis), or dental infection. • Sequela of orbital trauma (e.g., orbital fracture, penetrating trauma, retained intraorbital foreign body). • Sequela of eyelid, orbital, or paranasal sinus surgery. • Sequela of other ocular surgery (less common). • Vascular extension (e.g. , seeding from a systemic bacteremia or locally from facial cellulitis via venous anastomoses). • Extension from a septic cavernous sinus thrombosis.
- 9. ORGANISMS • Adult: Staphylococcus species, Streptococcus species, Bacteroides species. • Children: Haemophilus influenzae (rare in vaccinated children). • Following trauma: Gram-negative rods. • Dental abscess: Mixed, aggressive aerobes and anaerobes. • Immunocompromised patients (diabetes, chemotherapy, HIV infection): Fungi including those that produce zygomycosis infections (e.g. , Mucor) and Aspergillus.
- 10. • Laboratory studies: CBC with differential and blood cultures. • Gram stain and culture of any drainage (e.g. , blood and chocolate agars, Sabouraud dextrose agar, thioglycolate broth) • Tissue biopsy • Chest X-ray • Antinuclear antibodies • Serum IgG and IgG 4 levels INVESTIGATION
- 11. TREATMENT CONTINUE.. • Admit the patient to the hospital and consider consultation with infectious disease, otorhinolaryngology, neurosurgeon for suspected meningitis and oral maxillofacial surgeon for dental infection. • Broad-spectrum intravenous antibiotics to cover gram-positive, gram-negative, and anaerobic organisms are recommended for 48 to 72 hours, followed by oral medication for at least 1 week. The specific antibiotic agents vary. • In patients from the community with no recent history of hospitalization, nursing home stay, or institutional stay, recommendations are: • Ampicillin–sulbactam 3 g i.v. q6h in adults; 300 mg/kg per day in four divided doses in children, maximum daily dose 12 g ampicillin–sulbactam (8 g ampicillin component) or Piperacillin–tazobactam 4.5 g i.v. q8h or 3.375 g q6h in adults; 240 mg of piperacillin component/kg/day in three divided doses in children, maximum daily dose 18 g piperacillin.
- 12. • In patients suspected of harboring hospital-associated methicillin-resistant Staphylococcus aureus (HA-MRSA) or in those with suspected meningitis, add concurrent intravenous vancomycin at 15 mg/kg q12–24h in adults with normal renal function and 40 mg/kg per day in two or three divided doses in children, with a maximum daily dose of 2 g. For adults who are allergic to penicillin but can tolerate cephalosporins, use vancomycin as dosed above plus: Ceftriaxone 2 g i.v. daily and metronidazole 500 mg i.v. q6–8h (not to exceed 4 g per day). • For adults who are allergic to penicillin/cephalosporin, treat with a combination of a fluoroquinolone (for patients >17 years of age, moxifloxacin 400 mg i.v. daily or ciprofloxacin 400 mg i.v. q12h or levofloxacin 750 mg i.v. daily) and metronidazole 500 mg i.v. q6–8h. • Nasal decongestant spray as needed for up to 3 days. Nasal corticosteroid spray may also be added to quicken the resolution of sinusitis. TREATMENT CONTINUE..
- 13. • Erythromycin or bacitracin ointment q.i.d. for corneal exposure and chemosis if needed. • If the orbit is tight, an optic neuropathy is present, or the IOP is severely elevated, immediate canthotomy/cantholysis may be needed. • The use of systemic corticosteroids in the management of orbital cellulitis remains controversial. If systemic corticosteroids are considered, it is probably safest to wait 24 to 48 hours until an adequate intravenous antibiotic load has been given (three to four doses). • Mark extent of skin inflammation to monitor status. • Regular review of orbital and visual functions. • ENT to assess for sinus drainage (required in up to 50% of adults). • If any deterioration, repeat CT to exclude abscess formation. • orbital abscess, consideration should be given to urgent surgical drainage, especially with visual compromise or progression of clinical signs. TREATMENT