1. Prevalence and clinical
significance
In the UK, the 1998 and 2009 Adult Dental
Health Surveys indicated that within 11
years the incidence of tooth surface loss
(TSL) had increased by 10% and stated that
‘moderate tooth wear in 16- to 34-year-olds
is of clinical relevance as it is suggestive of
rapid tooth wear.’
As more patients retain teeth longer, TSL
represents a growing restorative and
aesthetic challenge.
TSL should be considered normal.
However, it may be considered pathological
if:
• The rate of loss is rapid or excessive
• The long-term survival of the dentition
becomes questionable
• The long-term survival of individual teeth
becomes questionable
• Teeth may become technically difficult to
restore if they deteriorate further
• It becomes a concern for the patient
• Dentine is exposed.
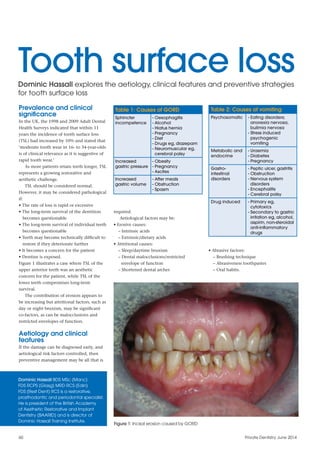
Figure 1 illustrates a case where TSL of the
upper anterior teeth was an aesthetic
concern for the patient, while TSL of the
lower teeth compromises long-term
survival.
The contribution of erosion appears to
be increasing but attritional factors, such as
day or night bruxism, may be significant
co-factors, as can be malocclusions and
restricted envelopes of function.
Aetiology and clinical
features
If the damage can be diagnosed early, and
aetiological risk factors controlled, then
preventive management may be all that is
required.
Aetiological factors may be:
• Erosive causes:
– Intrinsic acids
– Extrinsic/dietary acids
• Attritional causes:
– Sleep/daytime bruxism
– Dental malocclusions/restricted
envelope of function
– Shortened dental arches
• Abrasive factors:
– Brushing technique
– Abrasiveness toothpastes
– Oral habits.
Table 2: Causes of vomiting
Psychosomatic - Eating disorders;
anorexia nervosa,
bulimia nervosa
- Stress induced
psychogenic
vomiting
Metabolic and
endocrine
- Uraemia
- Diabetes
- Pregnancy
Gastro-
intestinal
disorders
- Peptic ulcer, gastritis
- Obstruction
- Nervous system
disorders
- Encephalitis
- Cerebral palsy
Drug induced - Primary eg,
cytotoxics
- Secondary to gastric
irritation eg, alcohol,
aspirin, non-steroidal
anti-inflammatory
drugs
Figure 1: Incisal erosion caused by GORD
Tooth surface lossDominic Hassall explores the aetiology, clinical features and preventive strategies
for tooth surface loss
Dominic Hassall BDS MSc (Manc)
FDS RCPS (Glasg) MRD RCS (Edin)
FDS (Rest Dent) RCS is a restorative,
prosthodontic and periodontal specialist.
He is president of the British Academy
of Aesthetic Restorative and Implant
Dentistry (BAARID) and is director of
Dominic Hassall Training Institute.
60 Private Dentistry June 2014
Table 1: Causes of GORD
Sphincter
incompetence
- Oesophagitis
- Alcohol
- Hiatus hernia
- Pregnancy
- Diet
- Drugs eg, diazepam
- Neuromuscular eg,
cerebral palsy
Increased
gastric pressure
- Obesity
- Pregnancy
- Ascites
Increased
gastric volume
- After meals
- Obstruction
- Spasm
2. Erosive causes
Intrinsic acids
This is due to voluntary or involuntary
regurgitation of acids and is more
damaging than extrinsic acids. Such
patients should be considered at high risk
of rapid progression of the erosion.
Involuntary regurgitation
Gastro-oesophageal reflux disease
(GORD) may have a variety of causes (see
Table 1).
The pattern of TSL for GORD tends to
affect the whole mouth. Generally, the
occlusal surfaces are most severely
affected due to attritional affects, as
illustrated in Figures 2 and 3.
Symptoms are not reliable indicators,
as patients with long-standing GORD
may be symptom-free and erosion may
be the only sign. Conversely, patients can
be sensitive to small amounts of acid.
Signs/symptoms may include:
• Heartburn
• Retrosternal discomfort/epigastric pain
• Dysphagia and pain on swallowing (hot
fluids in particular)
• Chronic cough
• Globus (feeling a ‘lump’ in the throat)
• Hoarseness/chronic laryngitis
• Asthma.
Voluntary regurgitation
Voluntary regurgitation may be
spontaneous or self-induced and be
associated with various conditions (see
Table 2).
This may present initially as perimolysis
where the erosive lesion is localised to the
palatal surfaces of the anterior maxillary
teeth. The tongue directs gastric contents
forwards and the lateral spread of the
tongue protects the lower teeth. Eventually,
as the enamel becomes unsupported, the
incisal edges may chip and fracture. Figures
4 and 5 illustrate a bulimic case with these
features.
Rumination
Subjects deliberately reflux gastric contents
and chew this before re-swallowing.
Preventive management of GORD and
reflux
Patients should be sympathetically
questioned, as they may be secretive
especially if there is an eating disorder or
alcohol abuse. It is helpful to repeat the
history at a subsequent appointment when
the patient has had time to reflect.
To estimate the activity of the TSL, the
patient should be questioned if they feel
their teeth have become shorter, thinner or
worn within the last year or five years.
Referral to a general medical practitioner/
gastroenterologist maybe indicated:
• If symptoms interfere with quality of life
• If there have been previous investigations
for reflux and the tests were inconclusive/
borderline and erosion is severe
• If, after eliminating dietary factors and a
period of review, erosion continues
• When there is no other obvious cause of
severe erosion.
If there is an eating disorder, patients require
medical help and psychological counselling.
Patient confidentially should be respected
all times.
Rinsing with fluoride after acid exposure
helps to neutralise the acid environment
and brushing should be avoided for one
hour to reduce abrasion.
Photographs are essential and should be
taken not only to aid in monitoring but also
to assist in co-diagnosis and compliance
with management strategies.
Extrinsic/dietary acids
Dietary practices/habits can significantly
impact on TSL (Table 3 lists some erosive
food and drinks).
Soft drinks (carbonated and still) have
seen a considerable increase in
consumption. It is also the titratable acidity
of drinks that is important in erosion, not
just the pH. Alcoholic beverages have
erosive potential but may also be linked
with reflux.
Private Dentistry June 2014 61
Clinical excellence
Table 3: Potentially erosive foods
and drinks
Potentially
erosive
drinks
- Soft drinks
- Sweetened and
non-sweetened
- Carbonated and
non-carbonated
- Fruit juices and fruit
flavoured drinks
- Sports and energy
drinks
- Some herbal teas
- Alcoholic drinks
Potentially
erosive
foods
- Fresh acidic fruit when
eating large quantities/
frequency (eg, grapes,
apples and citrus fruits)
- Vinegar/vinegar-based
foods and sauces (eg,
salt and vinegar crisps
and pickled foods)
- Tomato ketchup
- Fruit based sweets
(sweetened and
non-sweetened)
Figure 2: TSL of lower occlusal surfaces
caused by GORD
Figure 3: TSL on upper occlusal surfaces
Figure 4: Palatal erosion upper anteriors
caused by bulimia
Figure 5: Absence of TSL on posterior teeth
3. Oral hygiene products and habits
It should be established if the patient is
using a non-abrasive toothpaste and
atraumatic brushing technique and
appropriate advice given.
Attritional causes
Parafunction
Between eight and 20% of the population
may be affected by sleep bruxism while
20% may be affected by daytime bruxism.
Sleep studies confirm bruxism as a
central nervous system (CNS) sleep-
related movement disorder. Daytime
bruxism is likely to be more stress related.
Here the clenching may be more vertical,
while in sleep bruxism it may be more
lateral.
All bruxism patients are considered
high-risk due to the excessive amount of
time the teeth come into contact and the
excess bite forces generated.
Possible indicators of parafunction
may include:
• Fracture of teeth/restorations
• Parafunction reported by partner
• Patient aware day bruxism
• Muscle pain (particularly on waking) or
trismus
• Waking with an awareness of the teeth
• Soft tissue trauma/changes cheeks/
lateral border of the tongue.
Great emphasis is placed on healthy
foods/drinks but certain healthy foods can
demonstrate significant erosive potential if
consumed in excess (Table 3).
It is not just the total consumption of
acidic dietary substances that is important,
but also frequency and timing of exposure
and tooth brushing practices.
Erosion on its own causes greater TSL
than attrition, but the two in combination
produce more destruction.
Preventive management of extrinsic acids
A diet history should be taken over a
four-day period, including the weekend. All
foods and drinks should be recorded,
including quantity, frequency and habits. A
retrospective long-term dietary history is
often revealing.
Dietary counselling must be tailored to
the individual but may include:
• Limit acidic food and drinks to mealtimes
• Reduce frequency of acidic insults
• Finish meals with alkaline foods such as
cheese or milk
• Avoid acidic foods and drinks last thing at
night
• Avoid habits such as prolonged sipping
and holding acidic beverages in the
mouth and ‘frothing’
• Avoid brushing teeth for one hour after
acidic substances
• Check the pH of medication, foods and
drinks
• Chewing gum stimulates salivary flow and
increases buffering capacity
• Use low abrasivity toothpastes/atraumatic
brushing technique.
Environmental
These may include acid contact as part of
work or leisure activities. Battery, dynamite
and fertiliser factory workers, laboratory
technicians, professional wine tasters and
competitive swimmers may all be exposed.
Athletes may be more prone to erosion
as a result of dry mouth and excessive
consumption of low pH sports drinks.
Medication/drug taking
A number of common medications, such as
vitamin C tablets, aspirin and iron
preparations are acidic.
Figure 6: Frictional wear to anterior teeth
due to skeletal discrepancy
Figure 7: Shortened dental arch with
severe TSL
Figure 8: OPG illustrating shortened dental
arch
Figure 9: Upper occlusal view
Figure 10: Palatal view upper anteriors Figure 11: Lower incisors Figure 12: Patient smiling
62 Private Dentistry June 2014
4. A full examination of the TMJ, orofacial
muscles and occlusion is essential.
Management of parafunction
There does appear to be a link to stress,
particularly in daytime bruxism, but the
link with sleep bruxism is not clear.
Stress management has not shown
consistent/sustained improvement in the
condition.
Splints are indicated for all
parafunction patients and botulinum
toxin can have a role delivered into the
elevator masseter muscles, reducing
damaging effects, particularly where
hypertrophy has been identified.
Dental malocclusions/restricted
envelope of function
Malocclusions/restricted envelopes of
function may cause a predisposition to
TSL due to increased frictional forces.
This affects the anterior teeth in
particular.
Deep overbites and class III
malocclusions act as co-factors when
there is reduced posterior support,
erosive factors or bruxism. Crossbites
and lack of canine guidance can also
predispose. Orthodontics should be
considered.
Figure 6 illustrates a skeletal
discrepancy with a class III
Dominic Hassall will be speaking at
Dentistry LIVE on Saturday 14 June.
Taking place at the QEII Conference
Centre in London, Dominic will be
presenting ‘Restoration of the failing
dentition diagnosis, avoidance and
treatment’.
He will also be giving a hands-on
session entitled ‘Treatment planning
practical in restorative, implant and
aesthetic dentistry’ on Friday 13 June.
For more details, see page 52 or visit
www.dentistrylive.co.uk.
malocclusion, buccal crossbites and lack
of canine guidance on the left, resulting
in frictional wear to the anterior teeth.
Figures 7 and 8 illustrate a shortened
dental arch where there is also GORD that
has resulted in severe TSL.
Restricted envelopes of function
demonstrate a unique pattern of wear due
to its frictional nature. It affects the
palatal surfaces and incisal edges of the
upper anterior teeth and ceases at the
intercuspal contact point on the palatal
surface. This contrasts with erosion due to
vomiting, which erodes the entire palatal
surface of the upper anterior teeth. On the
lower incisor teeth, it is the incisal edges
and the facial aspect of the upper third of
the teeth that are affected.
The next two articles in this series will
consider the interventional and
restorative management if the patient
presents late or preventive strategies have
failed.
References
For the list of references that accompany
this article, email pd@fmc.co.uk. PD
Comments to Private Dentistry
@ThePDmag
Private Dentistry June 2014 63
Clinical excellence