
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Crf and dialysis
Similar to Crf and dialysis (20)
More from Darya Daoud
Recently uploaded
Recently uploaded (20)
Crf and dialysis
- 1. CRF and Dialysis Darya Osman Eman Salah Moaz Ahmed Manal Balla
- 2. Quick Overview of CRF Usually asymptomatic until advanced stages Usually detected at earlier stage by blood and urine test Common in individuals with: HTN DM Family history of CKD
- 3. Early Renal Disease – Renal Insufficiency
- 4. End Stage Renal Disease – Renal Failure
- 5. Indications for Dialysis Should be started when benefit of relieving uremic signs and symptoms outweighs risk and decrease in quality of life Indications vary for acute and chronic kidney injury
- 6. Dialysis indications for ARF Think AEIOU Acidemia – from metabolic acidosis Electrolyte abnormality e.g. severe hyperkalemia Intoxication acute poisoning with dialyzable SLIME substances (i.e. Salicylic acid, Lithium, Isopropanol, Mg containing laxatives and Ethylene glycol) Overload of fluid Uremia complications e.g. pericarditis, encephalopathy or GI bleeding
- 7. Dialysis indications for CRF Indicated when patient has symptomatic kidney failure and low glomerular filtration rate Studies found that early start of dialysis may be harmful Recently guidelines recommend deferring dialysis until a patient has definite kidney failure symptoms (i.e. those that occur at GFR of 5-9ml/min/1.732) May also be indicated if there is difficulty to medially control fluid overload or serum potassium level If symptoms of Intractable kidney failure may start dialysis at eGFR levels above 10ml/min/1.732
- 8. General Principles of Dialysis Works on the principles of diffusion and ultrafiltration of fluid across a semi- permeable membrane. Diffusion: movement of solute across semi- permeable membrane from region of high concentration to low concentration Ultrafiltration: water is driven by either a hydrostatic or an osmotic force is pushes through the membrane.
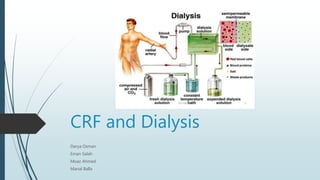
- 9. Principle of Dialysis Blood flows by one side of a semi-permeable membrane and a dialysate (special dialysis fluid) flows by the opposite side Semipermeable membrane contains pores of various sizes Smaller solutes and fluid pass through membrane but large substances do not (e.g. RBCs, large proteins) Replicates filtering process of the glomerulus of the kidney
- 10. Goal of Dialysis Solute clearance Diffusive transport (based on counter current flow of blood and dialysate) Conventional transport (solvent drag with ultrafiltration) Fluid removal
- 11. Types of Dialysis Haemodialysis Peritoneal Dialysis Hemofiltration
- 12. Hemodialysis Waste products are filtered from blood by a semi-permeable membrane and removed by the dialysis fluid, or dialysate. In-center: 4 hours, 3 days a week Home: Daily Nocturnal In-centre: 6-8 hours, 3nights/week
- 13. Types of Hemodialysis In center dialysis Home haemodialysis In centre nocturnal dialysis
- 14. Dialysate Composition Varies according to clinical need Major/Common components: High purified water Sodium Potassium Calcium Magnesium Chloride Bicarbonate dextrose
- 15. Access for Hemodialysis Arteriovenous Fistula Arteriovenous Graft Central Venous Catheter
- 16. Arteriovenous Fistula Preferred form of dialysis access once the fistula properly matures and gets bigger and stronger; it provides an access with good blood flow that can last for decades. Types: Radiocephalic (first choice) Brachiocephalic (second choice) Brachiobasilic (thirs choice, requires superficialization of basilic vein,i.e. Transposition)
- 19. Arteriovenous Graft Placed between an artery and a vein Either straight or looped Common sites: Radial artery to cephalic vein Brachial artery to cephalic vein Brachial artery to axillary vein Axillary artery to axillary vein
- 21. Central venous catheters Aka cuffed dialysis catheter Most commonly placed in the internal jugular Vein, existing at the upper, anterior chest. Can also be placed in the femoral vein. Subclavian catheters should be avoided due to risk of subclavian stenosis. ADV: no need for fistula. DIS ADV: short period use, infection, thrombosis, inadequate blood flow and overall increased risk of mortality.
- 23. Peritoneal Dialysis Use of peritoneal membrane as a filter to clear wastes and extra fluid from the body and to return electrolyte levels to normal. Peritoneal cavity: reservoir for dialysate (sodium, chloride, lactate and glucose) Peritoneum: semi- permeable membrane across which excess body fluid and solutes are removed (fluid, urea, creatinine and potassium)
- 25. Types of Peritoneal Dialysis Continuous ambulatory PD: 4-8 hours 4 times/day Automated PD: Continuous cycling once a day
- 26. PD Transport Diffusion Ultra-filtration Absorption
- 27. Advantages of Haemodialysis vs. Peritoneal dialysis Haemodialysis Done by trained health professionals who can watch for any problems. Allows contact with other people having dialysis, which may give you emotional support. Not done by oneself, as with peritoneal dialysis. Done for shorter amount of time and on fewer days each week than peritoneal dialysis. Peritoneal dialysis Gives you more freedom than hemodialysis. Can be done at home. You can do it when you travel. You may be able to do it while you sleep. You can do it by yourself. It doesn't require as many food and fluid restrictions as hemodialysis. It doesn't use needles.
- 28. Disadvantages of Hemodialysis vs. Peritoneal dialysis Hemodialysis Causes feeling of tiredness on the day of dialysis. Can cause problems such as low blood pressure and blood clots in the dialysis access. It increases your risk of bloodstream infections. Peritoneal diaysis Procedure may be hard for some people to do. Increases risk for an infection of the lining of the belly, called peritonitis.
- 29. Hemofiltration Based on convective transport rather than diffusion to remove solutes from blood of uremic patients Requires no dialysate, however require substitution fluid Positive hydrostatic pressure drives water and solutes get dragged along the flow of water Sometimes used in combination with hemodialysis Usually used for ARF and sepsis
- 32. Types of hemofiltration On-line intermittent hemofiltration (IHF) or hemodiafiltration (IHDF) Continuous hemofiltration (CHF) or hemodiafiltration (CHDF)
- 33. On-line intermittent hemofiltration (IHF) or hemodiafiltration (IHDF) Given in outpatient dialysis units 3 or 4 times per week 3 – 5 hours per treatment Substitution fluid is prepared on-line from dialysis solution Solution is run through two sets of membranes to purify it before infusing directly into blood line.
- 34. Continuous hemofiltration (CHF) or hemodiafiltration (CHDF) Used as treatment for fluid overload Treatment usually 8 – 12 hours (SLEF – Slow Extended Hemofiltration) A.K.A. continuous veno-venous hemofiltration No on-line creation of replacement fluid from dialysis solution Native hemodialysis access (i.e. fistulas or grafts) are unsuitable because of prolonged residence of access needles required might damage accesses
- 35. Advantages of Hemofiltration Convection overcomes reduced removal rate of larger solutes (due to slow speed of diffusion) Characterized by increased solute removal capabilities for higher MW solutes More similar to glomeruli in the function of filtration. More suitable than Hemodialysis to some symptoms Resistant Hypertension Water Retention, Hypertension Heart Failure caused by high blood volume, Uremic Pericarditis, Acute Renal Failure Hepatic Coma.
- 36. Disadvantages of Hemofiltration price is higher than Hemodialysis due to the need of plentiful placement fluid Blood pressure during Hemofiltration is not easy to control and low pressure and high pressure may occur if the volume is in imbalance. The small products may be not removed as effectively as Hemodialysis. Therefore, which dialysis to choose depends on each patient’s individual condition
- 37. Thank you!