
Recommended
More Related Content
Similar to ANTIEPILEPTIC-DRUGS.pdf
Similar to ANTIEPILEPTIC-DRUGS.pdf (20)
Recently uploaded
Recently uploaded (20)
ANTIEPILEPTIC-DRUGS.pdf
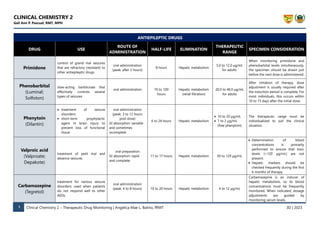
- 1. CLINICAL CHEMISTRY 2 Gail Ann P. Pascual, RMT, MPH 1 Clinical Chemistry 2 – Therapeutic Drug Monitoring | Angelica Mae L. Balino, fRMT 3D | 2023 ANTIEPILEPTIC DRUGS DRUG USE ROUTE OF ADMINISTRATION HALF-LIFE ELIMINATION THERAPEUTIC RANGE SPECIMEN CONSIDERATION Primidone control of grand mal seizures that are refractory (resistant) to other antiepileptic drugs oral administration (peak: after 2 hours) 8 hours Hepatic metabolism 5.0 to 12.0 µg/mL for adults. When monitoring primidone and phenobarbital levels simultaneously, the specimen should be drawn just before the next dose is administered. Phenobarbital (Luminal; Solfoton) slow-acting barbiturate that effectively controls several types of seizures oral administration 70 to 100 hours Hepatic metabolism (renal filtration) 20.0 to 40.0 µg/mL for adults After initiation of therapy, dose adjustment is usually required after the induction period is complete. For most individuals, this occurs within 10 to 15 days after the initial dose. Phenytoin (Dilantin) • treatment of seizure disorders; • short-term prophylactic agent in brain injury to prevent loss of functional tissue oral administration (peak: 3 to 12 hours post dose) GI absorption: variable and sometimes incomplete 6 to 24 hours Hepatic metabolism • 10 to 20 μg/mL • 1 to 2 μg/mL (free phenytoin) The therapeutic range must be individualized to suit the clinical situation. Valproic acid (Valproate; Depakote) treatment of petit mal and absence seizures oral preparation GI absorption: rapid and complete 11 to 17 hours Hepatic metabolism 50 to 120 μg/mL • Determination of blood concentrations is primarily performed to ensure that toxic levels (>120 μg/mL) are not present. • Hepatic markers should be checked frequently during the first 6 months of therapy. Carbamazepine (Tegretol) treatment for various seizure disorders; used when patients do not respond well to other AEDs. oral administration (peak: 4 to 8 hours) 10 to 20 hours Hepatic metabolism 4 to 12 μg/mL Carbamazepine is an inducer of hepatic metabolism, so its blood concentrations must be frequently monitored. When indicated, dosage adjustments are guided by monitoring serum levels.
- 2. CLINICAL CHEMISTRY 2 Gail Ann P. Pascual, RMT, MPH 2 Clinical Chemistry 2 – Therapeutic Drug Monitoring | Angelica Mae L. Balino, fRMT 3D | 2023 Ethosuximide (Zarontin) controlling petit mal seizures oral preparation (peak: 2 to 4 hours) 40 to 60 hours Hepatic metabolism; Renal filtration (20%) 40 to 100 μg/mL TDM for ethosuximide is performed to ensure that blood concentrations are in the therapeutic range Felbamate (Felbatol) use in severe epilepsies such as in children with the mixed seizure disorder, Lennox- Gastaut syndrome, and in adults with refractory epilepsy oral preparation GI absorption: nearly complete (peak: 1 to 4 hours) 14 to 22 hours in adults Renal and Hepatic metabolism 25 to 60 μg/mL Hepatic metabolism is enhanced by enzyme inducers such as phenobarbital, primidone, phenytoin, and carbamazepine and results in a decreased half-life. Gabapentin (Neurontin) monotherapy or in conjunction with other AEDs for patients suffering from complex partial seizures with or without generalized seizures and for pain management in some scenarios oral administration (peak: 2 to 3 hours) 5 to 9 hours in patients with normal renal function Renal infiltration 12 and 20 μg/mL Children require a higher dose than adults to maintain a comparable half-life as they eliminate the drug faster than adults. Lamotrigine (Lamictal) treat patients with partial and generalized seizures. oral preparation GI absorption: rapid and complete (peak: 3 hours) 15 to 30 hours Hepatic metabolism 2.5 to 15 μg/mL The rate of elimination is highly dependent on patient age and physiologic condition. Younger infants tend to metabolize this drug slower than older infants, and children metabolize lamotrigine twice as quickly as adults. Levetiracetam (Keppra) used in partial and generalized seizures oral administration (peak: 1 hour) 6 to 8 hours (increased in children and pregnant females and decreased in the elderly) Renal filtration 12.0 to 35.0 μg/mL lack of pharmacokinetic variability but may be useful in monitoring adherence and fluctuating concentrations during pregnancy Oxcarbazepine (Trileptal) treatment of partial seizures and secondarily in generalized tonic–clonic seizures oral administration (peak: 8 hours) 8 to 10 hours (adults) Hepatic metabolism 12 to 35 μg/mL Children have a higher clearance rate need a higher dosing regimen to obtain the optimal blood concentration compared with adults. In the elderly population, the drug
- 3. CLINICAL CHEMISTRY 2 Gail Ann P. Pascual, RMT, MPH 3 Clinical Chemistry 2 – Therapeutic Drug Monitoring | Angelica Mae L. Balino, fRMT 3D | 2023 clearance is reduced by 30%, so a lower dosage regimen is needed to maintain therapeutic concentrations. Tiagabine (Gabitril) treatment of partial seizures oral administration GI absorption: rapid and nearly complete (peak: 1-2 hours) 4 to 13 hours. Hepatic metabolism 20 to 100 ng/mL the ratio of free to bound drug is affected by other protein-binding drugs such as valproic acid, naproxen, and salicylates and by pregnancy. It is highly metabolized by the hepatic MFO pathway, so hepatic dysfunction can increase the half-life of the drug. Topiramate (Topamax) treatment of partial and generalized seizures oral administration (peak: 1-4 hours) 20 to 30 hours renal filtration; (some: hepatic metabolism) <25 mg/L The dose-to-blood concentration ratio in children is less than that of adults such that children require a higher dose to maintain plasma topiramate concentrations compared to adults. 13 Blood concentrations are increased secondary to renal insufficiency but may be decreased when used with other enzyme-inducing AEDs. Zonisamide (Zonegram) anticonvulsant used in adjunctive therapy for partial and generalized seizures oral administration GI absorption: 65% or higher (peak: 4-7 hours) 50 to 70 hours (px w/ monotherapy); 25 to 35 hours when other enzyme- inducing AEDs are administered concomitantly. Hepatic metabolism (acetylation; oxidation; glucuronide conjugation; renal excretion) 10 to 40 μg/mL Children require higher doses to achieve therapeutic blood concentrations compared to those of adults.
- 4. CLINICAL CHEMISTRY 2 Gail Ann P. Pascual, RMT, MPH 4 Clinical Chemistry 2 – Therapeutic Drug Monitoring | Angelica Mae L. Balino, fRMT 3D | 2023 PSYCHOACTIVE DRUGS DRUG USE ROUTE OF ADMINISTRATION HALF-LIFE ELIMINATION THERAPEUTIC RANGE SPECIMEN CONSIDERATION/ COMMENTS Lithium mood-altering drug primarily used in the treatment of bipolar disorder, recurrent depression, and aggressive or self-mutilating behavior, though it may also be used as a preventative treatment for migraines and cluster headaches oral administration GI absorption: rapid and complete (peak: 2-4 hours) 10 to 35 hours renal filtration 0.5 to 1.2 mmol/L Test tubes that contain lithium anticoagulants must be avoided to prevent falsely increased specimen results. Tricyclic Antidepressants to treat depression, insomnia, extreme apathy, and loss of libido oral administration GI absorption: variable (peak: 2-12 hours) 17 to 40 hours hepatic metabolism The rate of elimination can also be influenced by coadministration of other drugs that are eliminated by hepatic metabolism. Clozapine treatment of otherwise treatment- refractory schizophrenia oral administration GI absorption: rapid and complete (peak: 2 hours) 8 to 16 hours hepatic metabolism 350 to 420 ng/mL TDM may be indicated to check for adherence and in patients with altered pharmacokinetics. Olanzapine thienobenzodiazepine derivative that effectively treats schizophrenia, acute manic episodes, and the recurrence of bipolar disorders oral administration GI absorption: well (peak: 5-8 hours) fast-acting intramuscular (IM) injection 21 to 54 hours hepatic metabolism 20 to 50 ng/mL Estimated 40% is inactivated by first- pass metabolism.
- 5. CLINICAL CHEMISTRY 2 Gail Ann P. Pascual, RMT, MPH 5 Clinical Chemistry 2 – Therapeutic Drug Monitoring | Angelica Mae L. Balino, fRMT 3D | 2023 IMMUNOSUPPRESSIVE DRUGS DRUG USE ROUTE OF ADMINISTRATION HALF-LIFE ELIMINATION THERAPEUTIC RANGE SPECIMEN CONSIDERATION Cyclosporine suppression of host- versus-graft rejection of heterotopic transplanted organs oral administration GI absorption: 5-50% (peak: 1-6 hours) approximately 12 hours hepatic metabolism 100 to 400 ng/mL Erythrocyte content is highly temperature dependent; therefore, evaluation of blood cyclosporine concentrations requires rigorous control of specimen temperatures. Therefore, whole blood specimens are used to avoid this preanalytical variable. Tacrolimus immunosuppressive drug that is 100 times more potent than cyclosporine oral administration GI absorption: highly variable (peak: 1-3 hours) 10 to 12 hours hepatic metabolism 5–15 ng/mL Tacrolimus has been associated with thrombus formation at concentrations above its therapeutic range. Sirolimus antifungal agent with immunosuppressive activity that is used to prevent graft rejection in patients receiving a kidney transplant oral administration GI absorption: rapid (peak: 1-2 hours) 62 hours hepatic metabolism 4 to 12 μg/L (sirolimus + cyclosporine) 12 to 20 μg/L (sirolimus only) To increase the therapeutic efficacy, sirolimus is commonly co-administered with cyclosporine or tacrolimus as the bioavailability of sirolimus is 15% when taken in conjunction with cyclosporine. Everolimus prophylaxis of graft rejection in solid organ transplant shorter than sirolimus metabolized by CYP3A4 3 and 8 ng/mL Mycophenolic Acid lymphocyte proliferation inhibitor that is used most commonly as supplemental therapy with cyclosporine and tacrolimus in renal transplant patients. oral administration (peak: 1-2 hours) 17 hours renal excretion (>90%) 1 to 3.5 μg/mL Mycophenolate mofetil is a prodrug that is rapidly converted in the liver to its active form, mycophenolic acid (MPA). As with the other anti-rejection drugs, low trough concentrations of MPA increase the risk of acute rejection, while high concentrations imply toxicity.
- 6. CLINICAL CHEMISTRY 2 Gail Ann P. Pascual, RMT, MPH 6 Clinical Chemistry 2 – Therapeutic Drug Monitoring | Angelica Mae L. Balino, fRMT 3D | 2023 ANTINEOPLASTICS DRUG USE ROUTE OF ADMINISTRATION HALF-LIFE ELIMINATION THERAPEUTIC RANGE SPECIMEN CONSIDERATION/ COMMENTS Methotrexate an effective therapy for various neoplastic conditions oral administration (peak: 1 hour) 5 to 9 hours Renal filtration < 1 μmol/L 48 Trough serum specimens are preferred for determination of methotrexate concentrations. BRONCHODILATORS Theophylline (Theo-Dur, Theo-24, Uniphyl) treatment of respiratory disorders, such as asthma and stable chronic obstructive pulmonary disease, for patients that have difficulty using an inhaler or those with nocturnal symptoms oral administration (peak: 1 hour) Absorption can be variable, with peak blood concentrations achieved 1 to 2 hours after dosing when a rapid-release formation is administered or within 4 to 8 hours for a modified-release preparation 3 to 8 hours hepatic metabolism; renal filtration (20%) 10 to 20 µg/L There is a poor correlation between dosage and blood concentrations; however, TDM may initially be useful in optimizing the dosage or the confirmation of toxicity when suspected.