
Recommended
Recommended
More Related Content
What's hot
What's hot (19)
Similar to Editorial case report Ludwig Angina – The longest distance in this planet
Similar to Editorial case report Ludwig Angina – The longest distance in this planet (18)
More from Cecilia Young 楊幽幽
More from Cecilia Young 楊幽幽 (20)
Recently uploaded
Recently uploaded (20)
Editorial case report Ludwig Angina – The longest distance in this planet
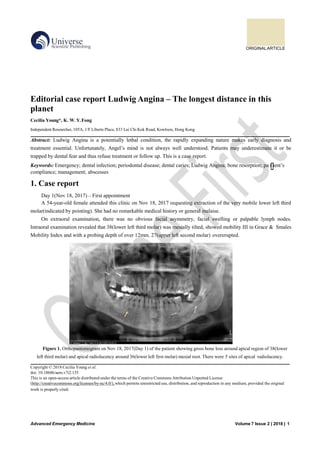
- 1. ORIGINALARTICLE Advanced Emergency Medicine Volume 7 Issue 2 | 2018 | 1 Editorial case report Ludwig Angina – The longest distance in this planet Cecilia Young*, K. W. Y.Fong Independent Researcher, 105A, 1/F Liberte Place, 833 Lai Chi Kok Road, Kowloon, Hong Kong Abstract: Ludwig Angina is a potentially lethal condition, the rapidly expanding nature makes early diagnosis and treatment essential. Unfortunately, Angel’s mind is not always well understood. Patients may underestimate it or be trapped by dental fear and thus refuse treatment or follow up. This is a case report. Keywords: Emergency; dental infection; periodontal disease; dental caries; Ludwig Angina; bone resorption; pa t ient’s compliance; management; abscesses 1. Case report Day 1(Nov 18, 2017) – First appointment A 54-year-old female attended this clinic on Nov 18, 2017 requesting extraction of the very mobile lower left third molar(indicated by pointing). She had no remarkable medical history or general malaise. On extraoral examination, there was no obvious facial asymmetry, facial swelling or palpable lymph nodes. Intraoral examination revealed that 38(lower left third molar) was mesially tilted, showed mobility III in Grace & Smales Mobility Index and with a probing depth of over 12mm. 27(upper left second molar) overerupted. Figure 1. Orthopantomogram on Nov 18, 2017(Day 1) of the patient showing gross bone loss around apical region of 38(lower left third molar) and apical radiolucency around 36(lower left first molar) mesial root. There were 5 sites of apical radiolucency. Copyright © 2018 Cecilia Young et al. doi: 10.18686/aem.v7i2.135 This is an open-access article distributed under the terms of the Creative Commons Attribution Unported License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 2. 2 | Cecilia Young etal. Advanced Emergency Medicine Figure 1. Orthopantomogram on Nov 18, 2017(Day 1) of the patient showing gross bone loss around apical region of 38(lower left third molar) and apical radiolucency around 36(lower left first molar) mesial root. There were 5 sites of apical radiolucency. Orthopantomogram(Figure 1) showed gross bone loss around apical region of 38 and apical radiolucency around 36 mesial root. Multiple apical radiolucencies were also found at other quadrants, respectively at 18(upper right third molar), 16(upper right first molar) and 45(lower right second premolar). First phrase treatment planning included extraction of the 38 and options of root canal treatment or extraction of 36. Treatment for other teeth would be planned later. Extraction of 38 was performed under local anesthesia with 2.5ml Xylestesin A(2% anhydrous lidocaine hydrochloride with 1:80000 adrenaline) by buccal infiltration & intraligamental infiltration. Socket was curetted and 1 Gelatemp sponge(9.5mg hardened gelatine and 0.5mg colloid silver) was packed to achieve hemostasis. Post-operative instructions were given verbally and in written notice(appendix I). Diclofenac sodium 25mg tds and famotidine 20mg bd, both for 5 days were prescribed. Day 3(Nov 20, 2017) – Second appointment Patient came back 2 days later complaining of progressive swelling in the face. On extra-oral examination, she had a mild swelling, erythema and tenderness in the lower left face, these signs were more intense in the submandibular area(figure 2 & 3), the submandibular region was very painful to palpation. Intra-oral examination revealed wound healing was normal. This diagnosis was early stage of Ludwig Angina. The potential airway blocking and lethal nature due to rapid progression if untreated were explained to the patient. However, she appeared unfazed and unworried(figure 4 & video 1). Patent refused routine management of referral to hospital and injection of antibiotics and thus operator decided to closely monitor the patient in clinic. First dose amoxicillin 500 mg and 250mg clavulanic acid(in two tablets of Augmentin 375mg), metronidazole 400mg, lysozyme HCL 20mg, famotidine 20mg and diclofenac sodium 25mg were given to the patient by oral administration. 5-day course of Augmentin 375mg tds, metronidazole 200mg tds lysozyme HCL 20mg tds, famotidine 20mg bd and diclofenac sodium 25mg tds were given. Chlorhexidine mouthrinse 10ml bd 90ml was also prescribed. The patient was instructed to have the second dose of all medication 4 hours and then to come back for review 5.5 hours after the initial dose of medication in clinic respectively. On review 5.5 hours later, the redness disappeared and the pain on palpation of submandibular space decreased. Figure 2. Frontal view of the patient on Nov 20, 2017(Day 3) showing mild lower left facial swelling.
- 3. Advanced Emergency Medicine Volume 7 Issue 2 | 2018 | 3 Figure 3. Side view on Day 3 showing diffuse lower left facial swelling with overlying erythema. Figure 4 & Video 1. The potential airway blocking and lethal nature due to rapid progression if untreated were explained to the patient but the patient appeared unworried and insisted in travelling to Japan. Day 5(Nov 22, 2017) – Third appointment On day 5 patient came back for review of the facial swelling. Examination showed that the left submandibular swelling had reduced but not yet completely subsided. Patient was explained to again that Ludwig Angina was a severe and potentially lethal condition and thus close monitoring and removal of all infective sources were required. However, the severity of the disease was disregarded again by the patient who had a plan of travelling to Japan the day after. The operator told the patient the cause of Ludwig Angina might be due to the non-vital 36 rather than 38 and therefore root canal treatment of 36 was advised. Patient refused it and operator instructed her to continue the medication prescribed. Oral and written information for root canal treatment were also given(appendix II). Another 5 days course of antibiotics(including Augmentin 375mg tds and metronidazole 200mg tds), lysozyme HCL 20mg tds and paracetamol 500mg qds were prescribed as backup. Patient was instructed to bring the backup medication to Japan, and to inform the operator with photos/videos via Whats app prior to taking the medication if the swelling and other symptoms did not subside completely or progress. A referral letter with the orthopantomogram attached was also given to the patient and the patient was told to seek care from dentists or physicians in Japan if her condition aggravated. Day 7(Nov 24, 2017) – Whats app communication Patient messaged the operator from Japan and complained of mild swelling which was not painful. She reported that she had already finished the course of medication prescribed on Day 3(Nov 20, 2017). The operator instructed her to take photos of her face in frontal and side views. The photos showed slight swelling in the left submandibular region. Patient was then advised to start the second course backup medication.
- 4. 4 | Cecilia Young etal. Advanced Emergency Medicine Figure 5. Frontal view of the patient on Nov 24, 2017(Day 7) showing slight mandibular facial swelling. Figure 6. Side view of the patient on Nov 24, 2017(Day 7) showing slight mandibular facial swelling. Day 10(Nov 27, 2017) – Whats app communication The operator asked the patient for updates of her condition via Whats app and informed her that the swelling should have been dealt with as soon as possible if it had not yet subsided completely. Patient replied that she had recovered already and the swelling was subsided. Patient confirmed that she did not need treatment. Day 11(Nov 28, 2017) – Whats app communication Consent of all clinical records including notes, photos and videos for teaching, oral health education and research purposes was obtained through Whats app. The operator informed the patient that the case was closed since the patient replied she did not need further treatment. The operator would not send further information to the patient unless upon request. 2. Discussion Karl Friedrich Wilhelm von Ludwig described the condition of Ludwig Angina without the name in 1836, as a rapidly progressive cellulitis with oedema of the soft tissues of the neck and floor of the mouth[1,2]. Majority of the cases are caused by odontogenic infections[3-5,12], most commonly involving mandibular second and third molars, due to the proximity of their roots with the submandibular fascial space, separated only by a thin inner
- 5. Advanced Emergency Medicine Volume 7 Issue 2 | 2018 | 5 cortex of the mandible[3,5]. Submandibular space is a potential space above the hyoid bone bounded antero-laterally by mandible, inferiorly by the superficial layer of deep cervical fascia and superiorly by the mucosa of the floor of mouth(and tongue)[6]. In this case, the orthopantomogram showed substantial bone loss around the apex of the 38. Apical radiolucency around the mesial root of 36 also indicates presence of infection at the periapical area. Persistence of infection of bone despite extraction of 38 and/or periapical infection of 36 were possible sources of infection that spread to the submandibular space, resulting in Ludwig angina. Infection of the submandibular space gives rise to edema, subsequently causing displacement of the floor of mouth and the tongue supero-posteriorly[6]. Without prompt intervention, airway can become compromised as cellulitis progresses, making it progressively difficult for clinicians to manage in a controlled setting, thus increasing the risk of mortality[3,7,9,13]. Treatment for Ludwig Angina typically includes maintenance of a patent airway[3,7,8,10,11-13] intensive antibiotic therapy[3,7,8,10,11-13] elimination of source of infection(e.g. root canal treatment, scaling and root surface debridement and extraction of the infected tooth)[3,8,10-12] and drainage[7,8,10-13]. Early diagnosis, close monitoring and maintenance of patient’s airway are essential. Intubation and tracheostomy may be needed when the airway is not secured[3,7,8,10-13]. In Hong Kong, patients with Ludwig Angina are best to be hospitalized due to the short travelling distance from private clinic to hospital and the emergency nature of the disease. Management of the patient in this case was however complicated by patient’s extreme underestimation of the disease’s severity. Her refusal of hospitalization for parenteral antibiotic therapy and insistence in travelling overseas, despite repeated explanation and advice, endangered herself and gave heavy pressure to the operator. Oral administration of antibiotics with empiric combination of amoxicillin clavulanate and metronidazole was prescribed. Amoxicillin clavulanate and metronidazole respectively targets gram-positive cocci and penicillin-resistant Bacteroides species, all of which have been reported to be involved in this polymicrobial infection[8,10,14-16]. Lysozyme hydrochloride was also administered as an adjunct agent for antibacterial and anti-inflammatory purposes[17]. The conservative medical therapy suppressed the swelling, but the low compliance of the patient and her refusal of further treatment ultimately caused the remaining of 4 apical radiolucencies i.e 4 sources of infection. Choy and Wong(2017) suggested that patient-related stresses greatly contribute to occupational stresses experienced by dentists in Hong Kong, and that dentists are advised to update their knowledge and skills to equip themselves for the increasing expectations and challenges from patients and society[18]. While it its integral for individual clinicians to equip themselves knowledge-wise and skill-wise for effective management of urgent and severe yet uncommonly encountered oral diseases like Ludwig Angina, these alone are not sufficient to treat the diseases due to low compliance of patients. Oral health education and promotion should be focused on how to combat patients’ underestimation of oral diseases and their avoidance of dental treatment due to fear and economic issue. 3. Conclusion Ludwig Angina is a relatively rare yet potentially fatal condition. Its rapidly progressive nature makes early diagnosis and prompt treatment essential. Treatment typically includes empiric antimicrobial administration, elimination of source of infection, drainage and close monitoring of the airway. Unfortunately, patients often underestimate the severity of oral diseases and delay seeking of treatment. Low compliance of patients inevitably pose challenges for clinicians to manage the disease. While it is of paramount importance for clinicians to become more knowledgeable and adept at managing such an unfamiliar yet lethal disease, it is perhaps even more crucial for practitioners and the government to educate the public the importance of oral health maintenance and regular dental checkups.
- 6. 6 | Cecilia Young etal. Advanced Emergency Medicine References 1. Von Ludwig WF. Über eine in neuerer Zeit wiederholt hier vorgekommene Form von Halsentzündung. Medicinisches Correspondenzblatt des Württembergischen ärztlichen Vereins 1836; 6: 21–25. 2. Burk J, Ludovici A. A translation together with biography of Wilhelm F von Ludwig. Bull Hist Med 1939; 7: 1115-1126. 3. Moreland LW, Corey J, Mckenzie R. Ludwig’s angina: Report of a case and review of the literature. Arch Intern Me 1988; 148(2): 461-466. 4. "Spitalnic SJ, Sucov A. Deep neck abscesses–changing trends. J. Emerg Med 1995; 13(4): 499-503. 5. Tschiassny K. Ludwig’s angina: An anatomic study of the role of the lower molar teeth in its pathogenesis. Arch Otolaryngol 1943; 38: 485-496. 6. Vieira F, et al. Deep Neck Infection. Otolaryngol Clin N Am 2008; 41: 459-483.Holland CS. The management of Ludwig's angina. Br J. Oral Surg 1975; 13(2): 153-159. 7. Srirompotong S, Art-Smart T. Ludwig’s angina: A clinical review. Eur Arch Otorhinolaryngol 2003; 260(7): 401-403. 8. Britt JC, Josephson GD, Gross CW. Ludwig’s angina in the pediatric population: Report of a case and review of the literature. Int J. Pediatr Otorhinolaryngol 2000; 52: 79–87. 9. Barakate M, Jensen M, Hemli J, et al. Ludwig’s angina: Report of a case and review of management issues. Ann Otol Rhinol Laryngol 2001; 110: 453-456. 10. Ocasio-Tascón ME, et al. Ludwig’s Angina: An uncommon cause of chest pain. Southern Medical Journal 2005; 98(5): 561-563. 11. Bross-Soriano D, et al. Management of Ludwig’s angina with small neck incisions: 18 years experience. Otolaryngology–Head and Neck Surgery 2004; 130(6): 712-717. 12. Finch RG, Snider GE Jr, Sprinkle PM. Ludwig's angina. JAMA 1980; 243(11): 1171-1173. 13. Rega AJ, Aziz SR, Ziccardi VB. Microbiology and antibiotic sensitivities of head and neck space infections of odontogenic origin. J Oral Maxillofac Surg 2006; 64(9): 1377-1380. 14. Rao DD, Desai A, Kulkarni RD, et al. Comparison of maxillofacial space infection in diabetic and nondiabetic patients. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010; 110(4): e7-12. 15. Poesch PW, Spusta L, Russmueller G, et al. Antibiotic susceptibility and resistance of the odontogenic microbiological spectrum and its clinical impact on severe deep space head and neck infections. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010; 110(2): 151-6. 16. Sava G. Pharmacological aspects and therapeutic applications of lysozymes. EXS 1996; 75: 433-449. 17. Choy HB & Wong MCM. Occupational stress and burnout among Hong Kong dentists. Hong Kong Med J 2017; 23(5): 480-488.
- 7. 楊幽幽牙科醫生 Dr. Cecilia Young Yau Yau 內容授權於原文醫藥人 以全篇原文為準 **以上內容已得病人同意使用作公共衛生教學用途 當中 "我們" 或 "示範中的方法" 指牙醫業內一般做法或其中一種 做法 內容只作一般公共衛生教育用途,病人應該與醫生商量自己的處 理方法。 所有牙醫均可進行公共口腔衛生教育,而公共衛生(Public Health )或社會牙醫科 (Community Dentistry )更是牙科內的一個科目。 牙醫專業守則 1.6 牙科/口腔健康教育活動 1.6.1 牙醫可以參與真確的牙科/口腔健康教育活動,例如演講 及作 專業發表.............. 1.6.3 向公眾提供的資料應具權威性、合宜並與一般經驗相符。 該等 資料應有事實根據、清楚易明及用詞淺白。 香港牙醫管理委員會 香港牙醫專業守則 http://www.dchk.org.hk/docs/code_c.pdf
- 8. 楊幽幽牙科醫生教育系列 以下為公共口腔衛生教育系列關鍵字 嵌塞 牙縫刷 腎病 致命牙齒脫位 膿 退縮 戒煙 骨質疏鬆 腫脹 四環素染色 楊幽幽牙科醫生 更薄的牙齒 刮舌板 牙齒長出 牙 齒不可逆性牙髓炎 水氟化 X光對生育期內婦女的影響, 什麼年紀最適合箍牙, 假牙, 傷口處理, 公共衛生教育, 剝牙, 副作用, 口腔種植, 成人矯齒成效如何, 止血, 正確刷牙及使用牙線方法, 楊幽幽牙科醫生口腔教育系列 注意事項, 洗牙流血點解, 活 動假牙托, 流血不止, 滿口牙套可以箍牙嗎, 漂牙, 牙周病, 牙周病患者是否可以箍牙. 透明牙箍有用嗎, 牙柱, 牙橋, 牙痛, 牙 瘡, 牙肉流血, 牙醫, 牙骹, 種牙, 空姐接觸的宇宙射線會否影響胎兒, 笑容, 箍牙會唔會失敗, 脫牙, 蛀牙, 關節 好唔好 以下為公共口腔衛生教育系列關鍵字, 阿士匹靈,抗血小板劑,抗凝血劑, 抗生素, 關節僵硬,銀粉, 矯正, 植牙, 膿腫, 研磨劑, 刷 蝕牙齒, 態度, ,撕脫, 乳齒, 細菌, 口氣, 咬, 矯正器, 腦膿腫, 刷牙, 緩衝作用, 過氧化尿素,齲齒,檢查,咀嚼, 複合, 牙套, 牙冠增 長手術, 環孢素A, 失智症, 牙,科, 牙橋, 牙科疾病, 牙科脫牙,牙科問題, 牙髓, 牙周膜, 牙菌膜, 矯齒,根管治療, 洗牙齒表面, 微電測試 牙髓, 預防性樹脂補牙, 玻璃離子, 牙腳尖, 二手煙, 敏感牙齒, 吸煙, 手術, 鑽洞測試,水銀, 成功,牙齒氟化, 發炎, 淋巴核, 神經, 牙齒過度長出酸鹼值, 維他命C, 智慧齒,華法林, 牙膏, 牙刷, 牙齒美白,牙齒漂白, 口氣, 失敗, 補牙, 牙線, 外觀, 咬合, 橋體, 牙冠,口腔種植周邊炎 , 含氟漱口水, 漱口水, 硝酸鉀, 口腔黏膜發炎, 尼古丁, 口腔疾病, 口腔感染, 預防, 牙袋, 家庭主婦, 感 冒, 象牙質, 牙齒創傷, 牙骨黏連, 牙周膜位置骨化, 磨蝕牙齒, 牙齒正畸, 氟素防蛀劑, 牙紋防蛀劑,鑲嵌物, 鑄造瓷貼片, 酸蝕 牙齒, 牙齒腫大, 漱口水, 肝素, 薄血藥, 維生素C,血栓栓塞, 國際標準化比值, 感染性心內膜炎, 琺瑯質, 局部麻醉劑, 三氯沙, 空間固定器, 進食次數,用餐次數, 全口假牙托、琺瑯質形狀缺陷,馬利蘭牙橋, 咽喉炎, 食物與牙齒健康, 奶瓶齲齒, 鎮靜, 牙 髓治療, 氟素凝膠, 牙腳斷裂, 牙腳吸收, 牙根整平術, 早期兒童蛀牙, 糖尿病, 效用, 測試, 牙齦, 牙齦組織, 牙齦出血, 雙氧水, 免疫抑制劑, 嵌塞, 牙縫刷, 腎病, 致命,牙齒脫位, 膿, 退縮, 戒煙,骨質疏鬆, 腫脹, 四環素染色, 更薄的牙齒, 刮舌板, 牙齒長出, 牙齒不可逆性牙髓炎, 水氟化X光對生育期內婦女的影響、什麼年紀最適合箍牙、假牙、傷口處理、公共衛生教育、剝牙、 副作用、口腔種植、成人矯齒成效如何、止血、正確刷牙及使用牙線方法、注意事項、洗牙流血點解、活動假牙托、流血 不止、滿口牙套可以箍牙嗎、漂牙、牙周病、牙周病患者是否可以箍牙. 透明牙箍有用嗎、牙柱、牙橋、牙痛、牙瘡、牙 肉流血、牙醫、牙骹、種牙、空姐接觸的宇宙射線會否影響胎兒、笑容、箍牙會唔會失敗、脫牙、蛀牙、關節, 常見的牙 患及預防方法, 蛀牙的成因及預防, 牙周病的成因及預防方法 甚麼是根管治療, 關於脫牙的事實, 銀汞合金安全嗎, 牙齒如何漂白, 需要矯齒的原因及準備, 牙齒創傷即時處理及治療, 懷 孕婦女需特別注重口腔健康, 如何除口氣, 骨質疏鬆與牙齒脫落的關係, 家長須助孩子護理乳齒, 牙周病─治療方法探究篇, 牙患可以致命, 鑲補牙齒方法知多少, 假牙扥 你們對我的期望合理嗎, 牙菌膜可以使種牙鬆脫, 糖尿病與牙周病互相影響, 必 先利其器 口腔衛生用品知多少, 脫牙前必須認真考慮, 預防蛀牙的方法氟素防蛀劑及牙紋防蛀劑, 漂白牙齒的各種方法, 細 數牙周病各種病徵, 用力刷牙≠清潔 使用漱口水是否好習慣, 吸煙與牙周病, 吸煙對治療牙周病的影響, 吸煙與口腔癌關係密切 戒煙為何與如何, 二手煙立法與自律, 乳齒對恆齒的影響, 公眾對洗牙的誤解調查, 兒童乳齒的根管治療, 第一隻長出的恆齒, 換牙時需注意事項, 護理口腔第一步正確刷牙方法, 敏感牙齒成因及預防, 公眾對洗牙的誤解應用篇, 如何保養活動假牙, 矯 齒點滴, 矯齒前應注意的事項, 木糖醇對人有害嗎, 口腔穿環的後遺問題, 牙周牙髓聯合症, 防敏感牙膏不適合長期使用, 頭 頸部放射治療前後的口腔護理, 幫助睡眠窒息症患者呼吸口腔矯治器, 根管治療時斷針是否失誤, 小朋友在牙科治療時不合 作, 嚴重蛀牙 幼兒一次被脫8隻乳齒(上) 嚴重蛀牙 幼兒一次被脫8隻乳齒(中), 嚴重蛀牙 幼兒一次被脫8隻乳齒(下), 香港牙膏並未含有「二甘醇」, 社會醫學研究電 話調查, 小朋友不肯見牙醫 怎辦?, 牙周病口瘡性潰痬與口腔癌 牙齒創傷幸與不幸, 智慧齒過度長出, 智慧齒過度長出引致 的其他牙患, 矯齒替代鑲假牙, 矯齒替代鑲假牙(二), 善用抗生素, 失去牙齒的其他後果, 一顆牙齒多個問題 根管治療後如何加上牙柱及牙套, 澳洲回顧研究 漱口水內的酒精致口腔癌, 牙齒美容 牙齒美容(二), 牙齒美容(三), 常見牙齒問題酸蝕, 牙科治療 為甚麼要磨蝕好的牙齒, 健康牙齒伴你一生, 淺談假牙的承扥問 題, 腎病患者的口腔問題, 抗凝血劑 抗血小板劑與脫牙
- 9. 感染性心內膜炎與牙科治療, 二手煙對兒童牙齒的影響, 失智症(老人痴呆症)與口腔健康 如何保持牙齒清潔, 防敏感牙膏新資訊, 牙套內會不會蛀牙, 探討牙科內常用的局部麻醉劑 孕婦及牙科常用藥物, 牙科病人與精神問題(上), 牙科病人與精神問題(下), 阻生智慧齒 殺菌劑三氯沙氾濫我們應否使用抗菌牙膏, 牙科病人的求診習慣, 診斷不同不知信那一個 什麼情況,什麼病人不宜脫牙, 關於植牙的種種迷恩, 如何處理長者的牙患, 預防牙患多角度孕婦與胎兒母親與嬰幼 兒, 牙周整形手術治敏感牙齒, 牙齦萎縮不能復原, 牙周組織再生法, 植骨與植牙手術 先植骨後植牙, 同時進行植骨 與植牙, 口腔植體周邊組織炎, 牙冠增長手術(上). 牙冠增長手術(下), 中小學教師與中學生對牙齒創傷認識不足, 牙 齒各類創傷與處理, 牙齒各類創傷與處理(2), 牙齒創傷當牙周膜死了, 牙齒創傷日後可能顯現的問題 牙齒創傷後的治療個案, 假牙可以戴多久, 即時性假牙托, 假牙的種類和設計, 假牙的種類和設計--種牙, 假牙的種 類和設計--牙橋, 假牙的種類和設計--活動假牙托, 我的牙齒為什麼不好, 由牙齒所引致的感染看似小事的牙瘡, 由 牙齒所引致的感染看似皮膚問題的牙瘡 由牙齒所引致的感染細菌進入眼部, 由牙齒所引致的感染細菌入腦, 由牙齒所引致的感染Ludwig氏咽峽炎阻塞氣道, 漱口水過酸易蛀牙, 食物與牙齒健康, 錯誤使用奶瓶餵飼幼兒奶瓶齲齒, 兒童嚴重蛀牙的治療方法, 兒童嚴重蛀牙的 治療方法--牙套, 牙齒咬合與移位(上), 牙齒咬合與移位(下), 智障人士的牙患, 智障人士如何預防牙患, 正確使用氨 素 氟素以外牙紋防蛀劑填補牙紋縫隙, 牙齒重疊最需要徹底清潔, 牙齒磨損, 對牙菌膜的監測 簡介牙髓的各種測試, 淺談口腔以外的牙科X光, 口腔以內的牙科X光, 牙髓死亡, 淺析咬合垂直距離, 牙痛, 到底哪 裡痛, 能不能忍一時之痛, 活動假牙托下不應有壞牙腳, 氟斑齒的處理方法 注意有否刷蝕牙齒, 牙齒消炎丸到底是 甚麼., 正確使用抗生素, 處理接近神經線的阻生智慧齒, 脫牙流血不止, 正確清潔牙齒及牙肉邊緣, 牙科手術儀器的 消毒程序, 牙科用具其他消毒程序, 黏液囊腫, 看見和看不見的蛀牙, 切除部分牙腳手術, 切除部分牙腳手術 2, 如何 清潔牙腳分岔位 上, 如何清潔牙腳分岔位 下, 牙線功能成疑, 美白牙膏去牙漬, 洗牙真的很痛嗎, 清刮牙腳, 再談清 刮牙腳, 洗牙流血只因牙肉發炎 口腔腫塊--牙齦瘤 口腔腫塊--乳突瘤, 口腔內的黑色素---牙齦的黑色素沉澱,G6PD缺乏症與牙科治療 頭頸癌放化治後牙科問題, 關愛基金改善政策使長者更受惠, 關愛基金改善政策使長者更受惠, 磨去蛀牙
- 10. Dr. Cecilia Young Yau Yau Oral Health Education series key words mellitus, diagnosis, early childhood caries, effectiveness, electric pulp test, enamel, erosion, esthetics, examination, extraction, failure, fever, fillings, fissure sealant, flight attendant, flossing, fluoride gel, fluorosis, gaps, gingiva, Gingival hypertrophy, gingival tissue, glass ionomer, gum bleeding, gum disease, halitosis, Heparin, housewife, hydrogen peroxide, hypoplasia, immunosuppressant, impaction, implant, infective endocarditis, inflammation, inlay, interdental brushing, international normalizing ratio INR, Kidney disease, lethal, local anaesthesia, look, luxation, lymph node, mechanical cleansing, mercury, mouthrinse, mucositis, nerve, nicotine, number of meals, nursing bottle syndrome, occlusion, onlay, oral disease, Oral Health Education, oral infection, orthodontic treatment, osteoporosis, overeruption, peri-implantitis, periodontal disease, periodontal membrane, pH value, plaque, pocket, pontic, porcelain veneer, post, post and core, potassium nitrate, prevention, abrasion、abrasives、abscess、abutment tooth、 aligners、amalgam、ankylosis、antibiotics、anticoagulation、antiplatelet、aspirin、 attitude、attrition、avulsion、baby teeth、bacteria、bad breath、biting、bleaching、 bleeding、bracing.., brain abscess、bridge、brushing、buffering effect、carbamide peroxide、caries、check-up、chewing、chlorhexidine、composite、crown、crown lengthening、cyclosporine A、dementia、Dental、dental bridge、dental decay、dental disesase. dental extraction、dental problem、dental pulp、dental scaling、dental trauma、dentine、denture、diabetes mellitus、diagnosis、early childhood caries、 effectiveness、electric pulp test、enamel、erosion、esthetics、examination、 extraction.. failure、fever、fillings、fissure sealant、flight attendant、flossing、fluoride gel、fluorosis、gaps、gingiva、Gingival hypertrophy、gingival tissue、glass ionomer、 gum bleeding、gum disease、halitosis、Heparin、housewife、hydrogen peroxide.. hypoplasia、immunosuppressant、impaction、implant、infective endocarditis、 inflammation、inlay、interdental brushing、international normalizing ratio INR、Kidney disease、lethal、local anaesthesia、look、luxation、lymph node、mechanical cleansing.. periodontal membrane、pH value、plaque、pocket、pontic、porcelain veneer、post、post and core、potassium nitrate、prevention、preventive resin restoration、pus、recession、removable appliance、removable denture、root apex.. Root Canal Treatment、root fracture、root planning、root resorption、scaling、second hand smoking、sensitive teeth、side effect、smile、smoking、smoking cessation、 successful、surgery、swelling、test cavity、tetracycline staining、thinner teeth. thromboembolism、tongue scrapper、tooth bleaching、Tooth bracing、tooth decay、 tooth eruption、tooth whitening、tooth. Irreversible pulpitis、toothache、toothbrush、 toothpaste、triclosan、vitamin C、warfarin、washing effect、water fluoridation.. wisdom tooth、wound handling ,complete Denture, space maintainer, Maryland Bridge ,pharyngitis, sedation , Pulpotomy. Small tooth, black tooth, damage tooth.