
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Amyloidosis: A Condition of Extracellular Protein Deposits
Similar to Amyloidosis: A Condition of Extracellular Protein Deposits (20)
Recently uploaded
Recently uploaded (20)
Amyloidosis: A Condition of Extracellular Protein Deposits
- 2. • Amyloidosis is a condition associated with a number of inherited and inflammatory disorders in which extracellular deposits of fibrillar proteins are responsible for tissue damage and functional compromise
- 4. fibrillar deposits bind proteoglycans and glycosaminoglycans abundant charged sugar groups in these adsorbed proteins gives deposit staining resemble starch (amylose). deposits are unrelated to starch.
- 5. • nonbranching fibrils, 7.5 to 10 nm in diameter, each formed of β-sheet polypeptide chains that are wound together misfolded proteins degraded intracellularly in proteasomes extracellularly by macrophages accumulate outside the cells
- 6. • two general categories: (1) normal proteins that have an inherent tendency to fold improperly, associate to form fibrils when they are produced in increased amounts (2) mutant proteins that are prone to misfolding and subsequent aggregation
- 7. • 3 most common amyloid : AL Amyloid : plasma cells made up of complete immunoglobulin light chains, the amino- terminal fragments of light chains, or both. a/w monoclonal B cell proliferation Defective degradation particular light chains are resistant to complete proteolysis
- 9. • The AA fibril : SAA AA (liver) IL-6 and IL-1 (inflammation) SAA monocyte-derived enzymes soluble end products a genetically determined structural abnormality in the SAA molecule itself renders it resistant to degradation by macrophages
- 10. • Aβ amyloid - cerebral lesions of Alzheimer disease. amyloid precursor protein (APP) -------- Aβ other proteins : Transthyretin (TTR) normal protein binds and transports thyroxine and retinol mutations - prone to misfolding and aggregation, and resistant to proteolysis. Familial amyloid polyneuropathies heart of aged persons (senile systemic amyloidosis) - structurally normal, but accumulates at high concentrations.
- 11. • β2-Microglobulin - component of MHC class I molecules and a normal serum protein, • fibril subunit (Aβ2m) in amyloidosis long-term hemodialysis retained in the circulation because it is not efficiently filtered through dialysis membranes.
- 13. On clinical grounds, systemic primary amyloidosis ------ associated with a monoclonal plasma cell proliferation secondary amyloidosis ------ complication of an underlying chronic inflammatory or tissue destructive process
- 14. • Primary - heart, gastrointestinal tract, respiratory tract, peripheral nerves, skin, and tongue • Secondary - kidneys, liver, and spleen • Gross - the organ is enlarged and the tissue typically appears gray with a waxy, firm consistency
- 15. On histologic examination, the amyloid deposition is always extracellular begins between cells, (often closely adjacent to basement membranes) As the amyloid accumulates, it encroaches on the cells ---destroy In the AL form ------ perivascular and vascular localizations are common.
- 16. STAINS
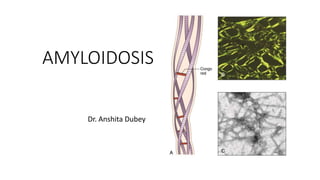
- 18. CONGO RED • FLUORESCENT DYE; NOT SPECIFIC FOR AMYLOID Staining – hydrogen bonding between congo red and B pleated sheet in a highly oriented linear and parallel manner. If the spatial configuration is altered-----------> reaction fails Postive birefringence- parallel arrangement of dye molecules
- 19. • Interpretations : AMYLOID – SALMON RED NUCLEI – BLUE UNDER POLARIZED LIGHT MICROSCOPE: AMYLOID : APPLE GREEN COLLAGEN : YELLOW RED
- 20. Principle : di azo dye which attaches itself parallel to the fibrils of amyloid and forms non polar hydrogen bonds- shows green birefringence of congo red stained amyloid under polarised light.
- 21. Lugols iodine
- 22. • Lugol’s Iodine - : Iodine 5% and KI 10% Iodine is not soluble in water, therefore KI I2 + I- ------------ I3- This makes a linear triiodide ion complex which is soluble. The triiodide ion slips into the coil of the starch causing an intense blue-black color
- 23. Metachromatic dyes Methyl/ crystal violet Toulidine blue • The dye reacts with the tissues to produce a color different from that of the original dye and from the rest of the tissue • It is attributed to stacking of dye cations at the sites of high density of anionic groups in the tissue. Stacking shortens the wavelength of maximum absorption • Substances that can be stained in this way are called chromotropes.
- 24. METHYL/ CRYSTAL VIOLET • Metachromatic stains negatively charged groups on the tissue + cationic dyes polymerization original colour of the dye changes to another colour Amyloid – purple red on a green background
- 25. TOLUIDINE BLUE Thiazine metachromatic dye with high affinity for acidic tissue components. Amyloid stains – weak basophilic
- 26. THIOFLAVIN T (fluorescent dye) • Thioflavin T is a benzothiazole salt • Dye interacts with the quaternary structure of B pleated sheet rather than with protein moieties, so binding is not dependent on any amino acid sequence. Acidic pH increases the selectivity by favouring the fluorochrome fraction binding to amyloid while depressing non amyloid fluorochrome staining. • In vivo and in vitro
- 27. ALCIAN BLUE • PRINCIPLE : polyvalent basic dye Forms salt linkages with acid groups of sulphated and carboxylated acid mucoploysaccharides • Amyloid deposits - Shades of green • Fibrin, muscle, cytoplasm – Yellow • Collagen, stroma - Red • Nuclei - Black
- 28. PAS stain Periodic acid oxidises the 1:2 glycol groups in the tissue to dialdehydes. Amyloid – light pink
- 29. HAEMATOXYLIN & EOSIN STAIN • HEMALUM (ALUMINIUM IONS & OXIDISED HAEMATOXYLIN) ---- NUCLEI • COUNTERSTAIN WITH AQUEOUS OR ALCOHOLIC SOLUTION OF EOSIN Y Amyloid - eosinophilic
- 30. IHC
- 31. P COMPONENT • Makes 10% of amyloid weight • Found on all amyloid fibrils except alzheimers senile plaques • Stabilizes fibril amyloid protein and decreases their clearance • Plays role in some of the special stains
- 32. KIDNEY most common and most serious feature of the disease Grossly – unchanged / may be abnormally large, pale, gray, and firm; in long-standing cases - may be reduced in size. Microscopically - the amyloid deposits are found in the glomeruli interstitial peritubular tissue & in the walls of the blood vessels.
- 33. • The glomerulus - focal deposits within the mesangial matrix and diffuse or nodular thickenings of the basement membranes of the capillary loops. the deposition encroaches on the capillary lumina - total obliteration of the vascular tuft The interstitial peritubular deposits amorphous pink casts within the tubular lumens walls of blood vessels - marked vascular narrowing.
- 34. SPLEEN • moderate or even marked enlargement (200 to 800 gm). • 2 PATTERNS – deposits limited to the splenic follicles, producing tapioca-like granules on gross examination (“sago spleen”)
- 35. involve the splenic sinuses, eventually extending to the splenic pulp, with formation of large, sheetlike deposits (“lardaceous spleen”) In both patterns, the spleen is firm in consistency.
- 36. LIVER GROSS - massive enlargement (9000 gm). Pale, grayish, and waxy on both the external surface and the cut section. MICRO - amyloid deposits first appear in the space of Disse adjacent hepatic parenchyma and sinusoids
- 37. HEART • systemic involvement - AL form. • The isolated form (senile amyloidosis) – older persons. minimal to moderate cardiac enlargement gray-pink, dewdrop-like subendocardial elevations(atrial chambers) histologic examination - throughout the myocardium myocardial fibers pressure atrophy
- 38. Clinical Course & Diagnosis • Nonspecific complaints - weakness, fatigue, and weight loss • Later - renal disease, hepatomegaly, splenomegaly, or cardiac abnormalities • Biopsy and subsequent Congo red staining is the most important tool • renal biopsy - urinary abnormalities Rectal and gingival biopsy specimens - generalized amyloidosis. Examination of abdominal fat aspirates stained with Congo red - simple, low-risk method. Bone marrow examination - plasmacytosis
- 39. THANK YOU