Androgen Insensitivity Syndrome (AIS) Explained
•Download as PPTX, PDF•
20 likes•13,361 views

1) Androgen Insensitivity Syndrome is a genetic condition where people have male chromosomes and male gonads but experience partial or complete feminization due to a mutation in the Androgen Receptor gene. 2) There are three main types - complete androgen insensitivity (CAIS) where external genitalia are fully female, partial androgen insensitivity (PAIS) where genitalia range from fully female to ambiguous, and mild androgen insensitivity (MAIS) with impaired sperm development. 3) Treatment involves hormone replacement therapy, psychological support, and potentially surgery to address medical issues or gender identity. Orchidectomy is usually recommended to prevent cancer risks.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Androgen Insensitivity Syndrome (AIS) Explained
Similar to Androgen Insensitivity Syndrome (AIS) Explained (20)
More from Dr. Aryan (Anish Dhakal)
More from Dr. Aryan (Anish Dhakal) (20)
Recently uploaded
Recently uploaded (20)
Androgen Insensitivity Syndrome (AIS) Explained
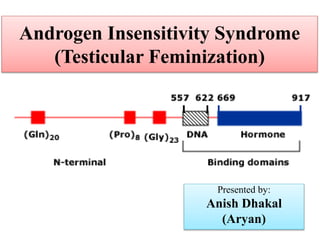
- 1. Androgen Insensitivity Syndrome (Testicular Feminization) Presented by: Anish Dhakal (Aryan)
- 2. Introduction Genetic condition where affected people have male chromosomes and male gonads with complete or partial feminization of the external genitals An inherited X-linked recessive disease with a mutation in the Androgen Receptor (AR) gene resulting in: Functioning Y sex chromosome Abnormality on X sex chromosome
- 3. Major Types: I. CAIS (completely insensitive to AR gene) External female genitalia Lacking female internal organs (Sertoli cells markers AMH and inhibin B present) II. PAIS (partially sensitive-varying degrees) External genitalia appearance on a spectrum (phenotypic women with mild virilization to phenotypic men with undervirilization and gynecomastia or infertility III. MAIS (mildly sensitive, rare) Impaired sperm development and/or impaired masculinization
- 4. Aetiology Peripheral receptors for testosterone absent or scanty they fail to respond to testosterone (defective/mutated receptors) In partial androgen insensitivity syndrome: Few receptors respond to testosterone External genitalia are of female phenotype Chromosome is XY
- 6. Clinical Features Gonads (testes) in the labia, or inguinal canal or intra-abdominal Maldeveloped testes Diagnosis: –Condition is not revealed until puberty –Positive family history –Childhood inguinal hernia discovers the testes
- 7. Clinical Features • Individual is typically feminine and tall • External genitalia looks female • Breast development is adequate • Nipples are small with pale areola • Pubic and axillary hairs are scanty or absent • Primary amenorrhea and or infertility • Vagina is short and blind
- 8. Clinical Features In partial androgen insensitivity syndrome: Signs of virilisation in a girl with primary amenorrhea Lack of virilisation in a boy
- 10. Bilateral labial gonads (testes) and short blind vagina in testicular feminization
- 11. A newborn genetic male (46, XY) with complete androgen insensitivity syndrome and female external genitalia 11 XY chromosome pattern but insensitivity to androgens
- 14. Investigations • Chromosomal study: Karyotype is 46, XY. • In infants and children, stimulation by hCG before measurement of hormones needed. • Serum testosterone is normal (or higher) • Serum E2 level is high normal for males • Serum LH level is normal or slightly elevated • FSH is normal. • USG: –Ovaries, uterus, upper 2/3rd of vagina and tubes are absent
- 15. Investigations • Confirmation of diagnosis is by gonadal biopsy • DNA sequencing for the AR gene is also possible though low probability for detetction in PAIS • Gonadal biopsy – Seminiferous tubules are small, hyalinized. – Spermatogenesis is absent. – Leydig cells and Sertoli cells are normal.
- 16. Differential diagnosis: Mullerian agenesis (for CAIS) Partial gonadal dysgenesis Defects in testosterone synthesis 17-beta-hydroxy steroid dehydrogenase type 3 deficiency (High level of androstenedione) 5-alpha reductase 2 deficiency (High ratio of testosterone to DHT)
- 18. Management • Medical care • Surgical care
- 19. Medical care • Hormone replacement therapy • Psychological aspect
- 20. Hormonal Replacement Therapy • Patient with complete androgen insensitivity – oestrogen replacement – progesterone not required because they have no uterus – has other benefits like osteoporosis prevention • Patient with incomplete androgen insensitivity – with male gender identity: testosterone and/or dihydrotestosterone (DHT) – With female gender identity: oestrogen
- 21. Current Guidelines for HRT: In women with CAIS or PAIS, guidelines suggest administration of oestrogen at the time of expected puberty, if gonadectomy was performed in childhood, or as soon as gonadectomy is performed after puberty However, testosterone therapy may also have advantages in some patients with proved CAIS with female identity
- 22. Psychological care • Most important aspect of medical care • Parents need genetic counseling to understand the nature of the condition and the risk of recurrence (25% for each subsequent pregnancy) as well as to identify other potential carriers • Whenever possible, obtain informed consent for any procedures or therapy • Any child, adolescent, or adult patient should receive age-appropriate information about the condition as well as psychological support • Sex assignment
- 23. Sex Assignment Usually assigned at birth with the expectation that future gender identity will develop in alignment with physical anatomy, initially assigned sex and rearing. Gender identity: Personal sense of one’s own gender Sex assignment of an intersex individual may also contradict their future gender identity Usually not attempted to change gender identity after age 3 unless requested by the patient (Possibility of gender dysphoria)
- 24. Surgical care • Orchidectomy – Standard care to prevent malignancy (3.4% at 25 years. Up to 33% at 50 years of age) – Malignant degeneration of testes – Timing of surgery is debatable, individual consideration is needed – If early: avoid raising uncomfortable psychosexual issues during adolescence or young adulthood – If late (teenage years or early 20s ): Allows pubertal development to occur spontaneously with the production of estrogen
- 25. Current Recommendations for Gonadectomy: • Gonadectomy be delayed until after the pubertal growth spurt and feminization in most subjects with CAIS • Gonadectomy might be recommended in female sex identity patients at the time of diagnosis of PAIS to prevent further virilization • If male sex is assigned in PAIS, no gonadectomy but surveillance is recommended • GnRH agonists might prevent undesired virilization in female identity patients if time is needed for counseling and decision making
- 26. Additional Treatment for PAIS with male gender identity: • Surgical correction of cryptorchidism in boys with PAIS soon after diagnosis to maintain testicular function and minimize the risk of malignancy • In males with PAIS, hypospadias repair might be undertaken at a younger age and mastectomy is appropriate for disfiguring persistent gynecomastia
- 27. • In female gender assigned patients with PAIS who have some degree of masculinization of the genitalia at birth, cosmetic reconstructive surgery. Use of vaginal dilators to stretch its length if sufficient length of vagina prevails Vaginoplasty –For those who desire marriage and unsatisfactory response from dilator therapy • Counseling: Reproductive function not possible
- 28. References: • Shaw’s Textbook Of Gynaecology ,16th edition • S. Peter, Pathogenesis and Clinical featires of disorders of androgen action, https://www.uptodate.com/contents/pathogen esis-and-clinical-features-of-disorders-of- androgen-action • M. Alvin et al, Diagnposis and treatment of disorders of androgen recpetors, https://www.uptodate.com/contents/diagnosis- and-treatment-of-disorders-of-the-androgen- receptor • DC DUTTA’ s textbook of gynecology, 7th edition
Editor's Notes
- Rarely diagnosed prior to puberty.
- Breast development is adequate because of estrogen derived from peripheral conversion of androstenedione. The gonads (Sertoli cells) secrete AMH (Anti-Müllerian hormone)
- Testicular feminization—bilateral inguinal gonads
- Bilateral labial gonads (testes) and short blind vagina in testicular feminization
- Upper 2/3rd of vagina, uterus and tubes are absent due to the effect of AMH