
Recommended
More Related Content
Similar to Contents lists available at ScienceDirect Journal of Affec
Similar to Contents lists available at ScienceDirect Journal of Affec (20)
More from AlleneMcclendon878
More from AlleneMcclendon878 (20)
Recently uploaded
Recently uploaded (20)
Contents lists available at ScienceDirect Journal of Affec
- 1. Contents lists available at ScienceDirect Journal of Affective Disorders journal homepage: www.elsevier.com/locate/jad Research paper The role of expressive suppression and cognitive reappraisal in cognitive behavioral therapy for social anxiety disorder: A study of self- report, subjective, and electrocortical measures Yogev Kivity⁎ ,1, Lior Cohen, Michal Weiss, Jonathan Elizur, Jonathan D. Huppert Department of Psychology, The Hebrew University of Jerusalem, Jerusalem, Israel A R T I C L E I N F O Keywords: Social Anxiety Emotion Regulation Cognitive Reappraisal Expressive Suppression Cognitive Behavioral Therapy A B S T R A C T Background: Contemporary models of cognitive behavioral therapy (CBT) for social anxiety disorder (SAD) emphasize emotion dysregulation as a core impairment whose
- 2. reduction may play a causal role in psy- chotherapy. The current study examined changes in use of emotion regulation strategies as possible mechanisms of change in CBT for SAD. Specifically, we examined changes in expressive suppression and cognitive reappraisal during CBT and whether these changes predict treatment outcome. Methods: Patients (n = 34; 13 females; Mean age = 28.36 (6.97)) were allocated to 16-20 sessions of CBT. An electrocortical measure of emotion regulation and a clinician- rated measure of SAD were administered monthly. Self-report measures of emotion regulation and social anxiety were administered weekly. Multilevel models were used to examine changes in emotion regulation during treatment and cross-lagged associations between emotion regulation and anxiety. Results: CBT led to decreased suppression frequency, increased reappraisal self-efficacy, and decreased un- pleasantness for SAD-related pictures (ps < .05). At post- treatment, patients were equivalent to healthy controls in terms of suppression frequency and subjective reactivity to SAD-related stimuli. Gains were maintained at 3- months follow-up. Decreases in suppression frequency and electrocortical reactivity to SAD-related pictures predicted lower subsequent anxiety but not the other way around (ps < .05). Lower anxiety predicted greater subsequent increases in reappraisal self-efficacy. Limitations: The lack of a control group precludes conclusions regarding mechanisms specificity. Conclusions: Decreased frequency of suppression is a potential mechanism of change in CBT for SAD. 1. Introduction Recent models of anxiety, including social anxiety disorder (SAD),
- 3. emphasize impairments in emotion regulation (Hofmann, Sawyer, Fang, & Asnaani, 2012; Morrison & Heimberg, 2013). Two regulation strategies, cognitive reappraisal and expressive suppression, may be particularly relevant for SAD (Morrison & Heimberg, 2013). In the process model of emotion regulation (Gross, 2015), cognitive re- appraisal is generally considered an adaptive strategy that involves cognitive change to regulate one's emotion – for example, attempts to reinterpret emotional stimuli in less threatening ways (Gross, 2015). On the other hand, expressive suppression is an attempt to inhibit one's expression of emotions and is generally considered maladaptive (Gross, 2015). In Heimberg's updated model (Morrison & Heimberg, 2013), emotion dysregulation in SAD includes avoidance of anxiety (e.g. avoidance or escape from stressful situations) and expressive suppres- sion due to believing that expressing emotions will lead to rejection or to excessive focus on oneself. The model further proposes that in- dividuals with SAD are less effective in implementing reappraisal. Ac- cordingly, decreased suppression and increased effective use of re- appraisal are hypothesized to lead to symptom reduction, for
- 4. example, by outward shifting of attention and by reducing exaggerated prob- ability and cost of rejection. Recently, studies have examined suppression and reappraisal in SAD (reviewed in Dryman & Heimberg, 2018). Cross-sectional and daily diary studies typically focus on the frequency of use of a strategy and self-efficacy (perceived success in implementation). Individuals with SAD report an over-reliance on suppression and lower frequency and self-efficacy of reappraisal (e.g., Farmer & Kashdan, 2012; https://doi.org/10.1016/j.jad.2020.10.021 Received 10 May 2020; Received in revised form 16 August 2020; Accepted 11 October 2020 ⁎ Corresponding author: Yogev Kivity, Department of Psychology, Bar Ilan University, Ramat Gan 5290002, Israel, Telephone: +972-3-5318715 E-mail address: [email protected] (Y. Kivity). 1 Yogev Kivity is now in the Department of Psychology, Bar Ilan University, Israel. Journal of Affective Disorders 279 (2021) 334–342 Available online 14 October 2020 0165-0327/ © 2020 Elsevier B.V. All rights reserved. T
- 5. http://www.sciencedirect.com/science/journal/01650327 https://www.elsevier.com/locate/jad https://doi.org/10.1016/j.jad.2020.10.021 https://doi.org/10.1016/j.jad.2020.10.021 mailto:[email protected] https://doi.org/10.1016/j.jad.2020.10.021 http://crossmark.crossref.org/dialog/?doi=10.1016/j.jad.2020.10 .021&domain=pdf Gaebler, Daniels, Lamke, Fydrich, & Walter, 2014). Impairments in frequency seem to be larger than impairments in self-efficacy in sup- pression while the opposite is true for reappraisal (Kivity & Huppert, 2018, 2019), thus supporting the Heimberg model. In addition, studies have also utilized subjective ratings during lab tasks of emotion regulation to study reappraisal and suppression abil- ities in SAD. These studies typically present SAD-related stimuli to participants, such as pictures of rejecting faces (Goldin et al., 2009a), pictures portraying scenes of rejection and embarrassment (Kivity & Huppert, 2016, 2018, 2019) and idiographic statements of negative self-beliefs (Goldin et al., 2009b) while asking participants to change the way they interpret these stimuli in order to reduce the distress they evoke in them. However, compared to questionnaires and daily diary measures, these lab studies have shown intact emotion
- 6. regulation abilities in SAD compared to controls, even under social stress (e.g., Gaebler et al., 2014; Kivity & Huppert, 2016, 2018, 2019). Thus, self- reported impairments are not reflected in lab performance. Among other possibilities, this discrepancy may suggest a difficulty im- plementing strategies in daily life despite an intact ability to implement them upon instruction in controlled circumstances, low ecological va- lidity of lab-based measures, or a bias in self-reports that does not exist in lab-based measures. Examining the role that each of these aspects (lab-based performance, self-reported frequency and self- reported self- efficacy) plays in treatments for SAD may shed light on their relative importance. Several techniques of cognitive behavioral therapy (CBT) for SAD seem relevant for improving emotion regulation. Psychoeducation and exposures likely decrease suppression, as patients learn that hiding their anxiety is futile and likely to backfire. Outward shifting of at- tention (focusing on the task at hand instead of on how one is per- ceived) presumably decreases suppression by decreasing patients’ pre- occupation with their overt signs of anxiety. Furthermore, cognitive
- 7. restructuring can potentially increase the use of reappraisal by chan- ging biased catastrophic cognitions. Finally, psychoeducation and in- vivo exposure challenge biased cognitions and are expected to promote reappraisal too. Studies have shown that self-reported reappraisal (frequency and self-efficacy) increases in CBT (Goldin et al., 2014a; Goldin, Morrison, Jazaieri, Heimberg, & Gross, 2017; Kocovski, Fleming, Hawley, Huta, & Antony, 2013; Moscovitch et al., 2012). However, findings regarding self-reported suppression are inconclusive, with one study reporting a decrease in frequency (Goldin et al., 2014a) and another reporting no change (Moscovitch et al., 2012). Less is known regarding lab- based measures: one study found improvements in reappraisal of negative social evaluations and negative self-beliefs during CBT (Goldin et al., 2013, 2014b). Importantly, the best test of the importance of emotion regulation as a treatment target for SAD is to examine its contribution to symptom improvement (Nock, 2007). Changes in reappraisal and suppression that predict treatment outcome would provide further support to Heimberg's model. Several studies found that increases in self-
- 8. reported frequency and self-efficacy of reappraisal predicted subsequent symptom reduction (Goldin et al., 2017; Kocovski, Fleming, Hawley, Ho, & Antony, 2015; Moscovitch et al., 2012), although another study found that only self-efficacy (but not frequency) of reappraisal pre- dicted subsequent outcome (Goldin et al., 2014a). Decreases in self- reported suppression frequency predicted contemporaneous, but not subsequent, symptoms reduction in one study (Goldin et al., 2014a) and did not predict outcome at all in another (Moscovitch et al., 2012). The only examination of lab-based reappraisal (Goldin et al., 2014b) found that greater changes in fMRI measures of reappraisal predicted greater symptom change during CBT for SAD, although subjective task per- formance did not. Thus, the self-report findings suggest that reappraisal increases during CBT for SAD and may be driving symptom change, with more consistent findings regarding self-efficacy than frequency. Additional studies are needed regarding lab-based emotion regulation. The present study examines changes in suppression and reappraisal during CBT for SAD and their role in treatment outcome using data from a previously completed study (Huppert, Kivity, Cohen,
- 9. Strauss, Elizur & Weiss, 2018). We collected weekly self-reports of the frequency and self-efficacy of reappraisal and suppression, and monthly lab-based measures of reappraisal and suppression in response to SAD- related pictures. Given past findings, our primary focus was self- reported self- efficacy of reappraisal and frequency of suppression. Frequency of re- appraisal and self-efficacy of suppression were of secondary interest. For the lab-based task, we focused on unpleasantness and event- related potentials (ERP) during reappraisal and suppression of SAD- related pictures. We focused on the late positive potential (LPP), an ERP with a posterior midline distribution and an onset of 300 ms post-sti- mulus (Proudfit, Dunning, Foti, & Weinberg, 2013). Larger LPP reflect sustained attention to stimuli and elaborative engagement in order to regulate the emotion (Proudfit et al., 2013). The LPP is sensitive to emotional intensity and to emotion regulation, with higher amplitudes for highly arousing stimuli that are reduced following instructions to regulate, including reappraisal and suppression, even within several seconds from the presentation of the stimuli (Proudfit et al., 2013). The LPP shows less habituation over repeated exposure to stimuli
- 10. compared to other psychophysiological measures (Proudfit et al., 2013), which allows for repetition of stimuli and attribution of changes in LPPs to the same stimuli as due to regulation. The LPP has been utilized in SAD (Kinney, Burkhouse, & Klump, 2019; Kivity & Huppert, 2018, 2019; Yuan et al., 2014) but we are unaware of studies examining it during CBT for SAD. We examined these hypotheses: 1) CBT will result in significant improvements in suppression and reappraisal, including reduced fre- quency of suppression and increased self-efficacy, frequency, and suc- cessful lab implementation of reappraisal. 2) Improvements in sup- pression and reappraisal will play a potentially causal role in CBT: improvements will predict subsequent improvements in anxiety and not vice versa. 3) We examined whether patients reached an equivalent level of emotion regulation to healthy controls (HCs) at post- treatment, and whether gains were maintained at 3-months follow-up without an a-priori hypothesis. 2. Method 2.1. Participants
- 11. Data were drawn from the CBT arm of a study of treatments for SAD (Huppert et al., 2018)2. Patients were recruited via advertisements and referrals. Participants were 34 patients who met DSM-IV-TR (American Psychiatric Association, 2000) criteria for SAD and 40 HCs with no history of psychiatric disorders, matched to patients on sex, age and education. One patient decided not to enter treatment and 5 HCs were removed because they did not have a continued low social anxiety score between screening and participation. The final sample included 33 patients (13 females, Age: 18-53, M = 28.36, SD = 6.97) and 35 HCs (15 females, Age: 19-45, M = 28.49, SD = 6.28). Participants were Hebrew speaking and family status was: single: CBT = 59%, HC = 61%; in a relationship: CBT = 41%, HC = 35%; divorced: CBT = 0%, HC = 4%. Education levels were: high school: CBT = 15%, HC = 29%; post-high school: CBT = 21%, HC = 9%; undergraduate degree/student: CBT = 42%, HC = 27%; graduate degree/student: 2 The original study also included participants receiving a computerized treatment for SAD called Attention Bias Modification. This treatment was of shorter duration compared to CBT, of a smaller sample size and only included three measurements of lab-based emotion regulation. In addition, group as-
- 12. signment was random only for a subset of the CBT patients. Due to these rea- sons, we decided not to include data from this treatment in the current study, which a priori was designed to examine the role of ER in CBT. Y. Kivity, et al. Journal of Affective Disorders 279 (2021) 334–342 335 CBT = 21%, HC = 26%. Groups did not differ on demographics (ps > .05). Ten SAD participants (29.41%) had one comorbid disorder and two (5.88%) had more than one. The most common comorbid disorders were depression (n = 9; 26.47%) or other anxiety disorders (n = 4; 11.76%). 2.2. Measures Liebowitz Social Anxiety Scale (LSAS; Liebowitz, 1987). A 24- item interviewer-rated measure of fear and avoidance of social inter- actions and social performance. The Hebrew version (Levin, Marom, Gur, Wechter, & Hermesh, 2002) was administered by trained clinical psychology doctoral students, blind to hypotheses. Internal consistency in all assessments was α = .90 – .96; interrater reliability for 15 ran-
- 13. domly chosen interviews was r = .94. Social Phobia Inventory (SPIN; Connor et al., 2000). A valid and reliable 17-item self-report measure of social anxiety symptoms, translated and back translated to Hebrew for previous studies. Internal consistency in all assessments was: α = .78 – .95. Emotion Regulation Questionnaire – Self-Efficacy and Frequency (ERQ; Gross & John, 2003). We used the reliable and valid Hebrew version (Carthy, Horesh, Apter, Edge, & Gross, 2010). Fol- lowing Goldin et al. (2009b), we measured both the frequency (ERQ-F) and self-efficacy (ERQ-SE) in social situations instead of frequency only (internal consistency of all subscales: α = .73 – .97). Items tap into reappraisal (e.g., “When I want to feel less negative emotion, I change the way I'm thinking about the situation”) and suppression (e.g., “I control my emotions by not expressing them”) which participants en- dorse using a 1 ("Seldom"/"Ineffectively") to 7 ("Often"/"Effectively") scale. Emotion Regulation Task. Full details are provided in supple- mental material, section 1. We used a task that was developed by Hajcak and Nieuwenhuis (2006) who presented emotionally- salient
- 14. pictures to participants and instructed them to either passively view the picture or to reappraise the emotion it evokes in them while ERP ac- tivity was recorded and unpleasantness ratings were collected. Hajcak and Nieuwenhuis found that the amplitude of the LPP and the level of subjective unpleasantness were decreased during reappraisal compared to passive viewing. Thus, the task is validated and suitable for studying the effects of emotion regulation on electrocortical activity and sub- jective unpleasantness. In the current study, we adapted the task to measure suppression in addition to reappraisal and used SAD- related pictures rather than general pictures (Kivity & Huppert, 2018, 2019). In selecting the stimuli for the task, we chose to focus on shame, embar- rassment and rejection because these experiences are central in SAD (Goldin et al., 2009b; Morrison & Heimberg, 2013; Moscovitch, 2009)3. Twenty trials of each condition were included: viewing of SAD- related pictures, viewing of neutral pictures, reappraisal of SAD-related pic- tures and suppression of SAD-related pictures. When viewing SAD-related pictures, participants imagined them- selves as the character that is the focus of shame, rejection, and em-
- 15. barrassment. When viewing neutral pictures, participants responded naturally. When reappraising, participants first imagined themselves as the character and then changed the way they think of the picture to decrease their unpleasantness (e.g., "This guy is not laughing at me, but at someone else"). When suppressing, participants first imagined themselves as the character and then concealed any expression of emotions. To enhance the effect of the suppression manipulation, a web camera was placed above the computer screen and participants were told that a member of the research team would review the recordings. Participants were instructed to avoid any expression of their emotions such that it would be impossible to tell whether they were viewing neutral pictures or concealing their emotions4. After each trial, participants rated their unpleasantness on a Self- Assessment Manikin (SAM; Lang, Bradley, & Cuthbert, 2008) scale (1 through 9; 5 being neutral; transformed such that higher ratings express greater unpleasantness). We focused on unpleasantness ratings in order to complement the LPP data (which is mostly correlated with arousal) and arrive at a more complete picture of the participants’
- 16. emotional experience that takes into account the two basic dimensions of emo- tions – valence and arousal. After providing unpleasantness ratings, participants were asked to indicate the instructions they followed during that trial. In the reappraisal condition, participants were also asked to record the new interpretation they came up with for the pic- ture (results not reported here). Ratings were averaged for each condition and a regulation score (view – regulate; calculated on the transformed scores) was calculated to capture the amount of reduction in unpleasantness. Higher scores indicate larger regulation effects. SAD-related pictures were collected from the internet5, normed and shown to evoke moderate shame, embarrassment, rejection and un- pleasantness (Kivity & Huppert, 2018, 2019). These depicted situations of shame, rejection, and/or embarrassment such as scenes of people pointed and laughed at, anxious people during a public speech, and facial expressions of contempt. Neutral pictures were taken from the International Affective Picture System (IAPS) database (Lang et al., 2008).
- 17. Psychophysiological Recording, Data Reduction, and Analysis. Full details are provided in section 2 of the supplement. ERPs were constructed by averaging trials in each condition (view, suppression, reappraisal and view neutral). Following Moser, Hartwig, Moran, Jendrusina, & Kross (2014), the LPP was quantified as the average voltage in 5 parietal electrodes (CPz, P1, Pz, P2, POz) in the entire segment (400-2000 ms). A regulation change score (view – regulate) was calculated to capture the amount of reduction in the LPP. Higher scores indicate larger regulation effects. Trials in which participants failed to use the instructed strategy were excluded (4.57% on average, no group differences). Studies have shown that the LPP can be reliably measured with as little as 8 trials and that it varies little beyond 12 trials (Moran, Jendrusina, & Moser, 2013). Assessments with fewer than 12 valid trials in each condition were removed from analyses (5% across groups, no group differences). 2.3. Treatment and therapists Individual CBT was delivered for up to 20 sessions using a manual by Roth-Ledley, Foa, & Huppert (2006), based on Clark's (2005) CBT for SAD. Components such as building an idiographic model,
- 18. outward shifting of attention, safety behaviors experiment, video feedback, be- havioral experiments and exposures, and optional use of imaginal ex- posure, assertiveness training, or social skills training are included. Therapists were four clinical psychology doctoral students with 2-4 years of CBT experience. Videorecordings of sessions were used in group supervision by the last author. 3 Shame, embarrassment and rejection are likely separate, but related, ex- periences. Similar to previous studies (e.g., Goldin et al., 2009), when designing and validating the task (Kivity & Huppert, 2018, 2019) we were not able to examine these experiences separately due to a small number of stimuli that purely fall into one of these categories. It remains for future studies to examine these experiences separately. 4 It should be noted that although the view condition is not entirely a passive one (as it includes perspective taking), it is still possible that i t requires less cognitive effort than the reappraisal and suppression conditions. However, studies have shown that cognitive effort alone does not explain the down-reg- ulatory effects of reappraisal (Foti & Hajack, 2008). 5 See a sample picture at
- 19. https://tinyurl.com/ShameArousingPicture. Y. Kivity, et al. Journal of Affective Disorders 279 (2021) 334–342 336 https://tinyurl.com/ShameArousingPicture 2.4. Procedure The institutional review board approved the study. After providing informed consent, participants were evaluated by trained independent evaluators (blind to hypotheses) using the Mini-International Neuropsychiatric Interview (Sheehan et al., 1998) and the LSAS. Par- ticipants completed a baseline assessment and entered treatment. Pa- tients completed the ERQ before and after each session (post- session ratings were of secondary interest and are only reported in Supple- mental Material, Section 4). Patients also completed in-lab assessments at pre-treatment, every four sessions during treatment, at post- treat- ment and at 3-months follow-up which included the LSAS, SPIN, ERQ, and the lab task. Thus, each patient had up to seven assessments (pre- treatment, sessions 4, 8, 12 and 16, post-treatment, and follow- up). HCs only completed a single assessment and were not followed long-
- 20. itudinally. Thus, HCs were included only in analyses of equivalency. 2.5. Data Analyses We used intent-to-treat linear multi-level models (assessments at level 1 repeated within patients at level 2) implemented in R package 'nlme' (Pinheiro, Bates, DebRoy, Sarkar, & R Core Team, 2016). In- cluding therapists as a third level showed negligible and non- significant effects (ICCs: Med = .00, range: 0 – 0.049) and therefore this level was removed. We used restricted maximum likelihood estimation, a first- order autoregressive level 1 covariance structure and random intercepts and slopes at level 2. For H1, linear rates of change were examined by including session/assessment number as a level 1 predictor (centered at pre-treatment). Intercepts represent estimated levels of the dependent variable at pre-treatment and slopes represent estimated changes in the dependent variable between two assessment points (one/four sessions, depending on the measure). To examine changes from post- treatment to follow-up we fitted a piece-wise model that examines changes during treatment and from post-treatment to follow-up separately. This was done by adding the follow-up data to the abovementioned model
- 21. and adding a dummy coded variable that captures post-treatment to follow- up changes (coded “1” for follow-up assessment and “0” for all other assessment). The fixed effect of the dummy variable expresses the amount and significance of the change from post-treatment to follow- up. H2 was examined by modeling within-patient variation in the pre- dictor following recommended procedures (Wang & Maxwell, 2015). Monthly scores of the predictor (patient mean-centered) served as within-patient scores in a cross-lagged (1-month) model. Within-subject effects represent cross-lagged associations between the predictor and the outcome. Per Wang and Maxwell (2015) we did not control for linear time effects as we wished to model and explain these very effects. Following Falkenström, Finkel, Sandell, Rubel, and Holmqvist (2017), we did not include the lagged dependent variable as a predictor because it introduces a dependency between the dependent variable and the error, thus violating assumptions. However, the first auto- regressive residual structure partly accounts for the effects of prior on current levels of the outcome. For consistency, we only analyzed
- 22. monthly scores of the SPIN and ERQ. A cross-lagged association was interpreted as significant only if effects were significant for clinician-rated and self- reported anxiety. For H3, comparisons were conducted using clinical equivalency procedures (Kendall, Marrs-Garcia, Nath, & Sheldrick, 1999) through t tests examining non-inferiority (i.e., < 1 SD difference) of post- treat- ment scores compared to HCs. A significant effect in noninferiority tests suggests that patients are non-inferior to HCs. Effect sizes were calculated as semi-partial r (rs; Jaeger, Edwards, Das, & Sen, 2016; Nakagawa & Schielzeth, 2013) using package 'r2glmm' in R (Jaeger & R Core Team, 2016). These represent the un- ique contribution above and beyond the contribution of other pre- dictors in the model and are presented in absolute values. 3. Results 3.1. Changes in regulation (H1) and equivalency to HCs (H3) 3.1.1. Change in self-reports Descriptive statistics for all study variables are presented in sup- plemental material, section 3. Changes are shown in Fig. 1. Suppression. Consistent with hypotheses, the frequency of sup-
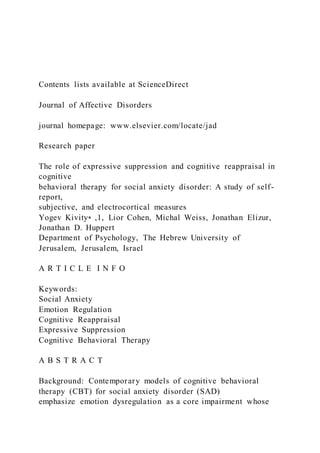
- 23. pression decreased during treatment (t467 = -3.98, p < .01, rs = .22 [.14, .30]) and did not change from post-treatment to follow-up (b = -.10, t490 = -.62, p = .53, rs = .01 [.00, .10]). In contrast to hypotheses, self-efficacy of suppression decreased during treatment (t467 = -2.85, p < .01, rs = .14 [.05, .22]) and did not change from post-treatment to follow-up (b = -.09, t490 = -.64, p = .52, rs = .01 [.00, .10]). Reappraisal. Consistent with hypotheses, self-efficacy of reappraisal increased during treatment (t467 = 3.67, p < .01, rs = .17 [.08, .25]) and did not change from post-treatment to follow-up (b = -.02, t490 = -.10, p = .92, rs = .00 [.00, .10]). In contrast to hypotheses, no changes in frequency of reappraisal were observed (t467 = .04, p = .97, rs = .00 [.00, .10]) nor did they change from post-treatment to follow- up (b = .08, t490 = .33, p = .74, rs = .01 [.00, .10]). 3.1.2. Change in lab-based measures Changes are shown in Fig. 2 and Fig. 3. View SAD-related pictures. As hypothesized, unpleasantness ratings decreased during treatment (t115 = 4.49, p < .01, rs = .28 [.13, .42]) and did not change from post-treatment to follow-up (b = .08, t138 = .70, p = .49, rs = .03 [.00, .18]). The LPP while viewing SAD- related pictures did not change significantly during treatment (b
- 24. = -.46, t103 = -1.80, p = .07, rs = .14 [.01, .30]) or from post-treatment to Fig. 1. Change in frequency and self-efficacy of reappraisal (top panel) and suppression (bottom panel) during Cognitive Behavioral Therapy (CBT). Error bars represent estimated standard errors. Only data from sessions 1-16 are presented because only 5 patients received more than 16 sessions. b = esti- mated weekly change in emotion regulation. ** p < .01 Y. Kivity, et al. Journal of Affective Disorders 279 (2021) 334–342 337 follow-up (b = 1.73, t126 = 1.11, p = .27, rs = .05 [.00, .20]). View neutral pictures. Supporting our hypotheses, we found no change in unpleasantness ratings during CBT or from post- treatment to follow-up (during: t115 = -.43, p = .67, rs = .04 [.00, .20]; post- treatment to follow-up: b = -.05, t138 = -.26, p = .79, rs = .02 [.00, .17]) and in the LPP (during: b = -.29, t103 = -1.04, p = .30, rs = .09 [.00, .25]; post-treatment to follow-up: b = 1.86, t126 = 1.09, p = .28, rs = .05 [.00, .20]) while viewing neutral pictures. Suppression. Examining suppression-related reductions in un-
- 25. pleasantness (compared to viewing pictures) we found that reductions were significantly different from zero at pre-treatment (b = .25, t115 = 3.84, p < .01), indicating that suppression was effective in down-regulating negativity. Consistent with hypotheses, regulation scores did not change during treatment (t115 = -1.77, p = .08, rs = .16 [.02, .31]) or from post-treatment to follow-up (b = .03, t138 = .29, p = .78, rs = .02 [.00, .18]). Reductions in LPP via suppression were not different from zero at pre-treatment (b = .69, t103 = 1.00, p = .32), suggesting that suppression was not effective in down regulating the LPP. Also consistent with hypotheses, regulation scores did not change during treatment (b = -.10, t103 = -.36, p = .72, rs = .03 [.00, .20]) and from post-treatment to follow-up (b = -.68, t126 = -.50, p = .61, rs = .03 [.00, .19]). Reappraisal. Reappraisal-related reductions in unpleasantness were significantly different from zero at pre-treatment (b = 1.41, t115 = 10.33, p < .01) indicating that reappraisal was indeed effective in down-regulating negativity. However, in contrast to hypotheses, we also found significant decreases in regulation scores during CBT (t115 = - 3.98, p < .01, rs = .26 [.11, .41] and no change from post- treatment to
- 26. follow-up (b = -.16, t138 = -1.25, p = .21, rs = .06 [.00, .21]). Additional analyses showed that raw unpleasantness ratings during reappraisal did not change (b = .02, t115 = .60, p = .55, rs = .03 [.00, .20]) which suggests that the decrease in regulation scores of re- appraisal was driven by a decrease in unpleasantness whi le simply viewing SAD-related pictures and not by a decrease in unpleasantness ratings during reappraisal. Fig. 2. Mean unpleasantness ratings while viewing neutral pictures and while viewing (top panel), suppressing, and reappraising (bottom panel) SAD-related pictures during Cognitive Behavioral Therapy. Higher scores indicate greater unpleasantness. Error bars represent estimated standard errors. Only data from sessions 1-16 are presented because only 5 patients received more than 16 sessions. b = estimated change in unpleasantness every four session. ** p < .01 Fig. 3. Picture-locked Event Related Potentials in the emotion regulation task pooled at parietal sites (CPz, P1, Pz, P2, POz), shown separately at pre- (top panel) and post- (bottom panel) cognitive behavioral therapy. Green, blue, red, and black lines represent amplitudes in the view neutral, reappraisal, suppression and view conditions, respectively. Y. Kivity, et al. Journal of Affective Disorders 279 (2021) 334–342
- 27. 338 When examining reappraisal-related reductions in the LPP, we found that reductions were not different from zero at pre- treatment (b = .52, t103 = .71, p = .48), indicating that reappraisal was not effective in down-regulating the LPP. Also, inconsistent with hy- potheses, regulation scores did not change during treatment (b = -.06, t103 = -.20, p = .84, rs = .02 [.00, .19]) and from post-treatment to follow-up (b = -1.66, t126 = -1.21, p = .23, rs = .10 [.01, .25]). 3.1.3. Equivalency to HCs Equivalency tests were only carried out for measures in which pa- tients showed impairments compared to HCs at baseline: self- report measures of emotion regulation and subjective unpleasantness while viewing SAD-related pictures (Kivity & Huppert, 2019). In terms of self- reported emotion regulation, at post-treatment, patients reached equivalency to HCs in terms of frequency and self-efficacy of suppres- sion (p < .01) but continued to show lower frequency and self- efficacy of reappraisal (ps > .05). In addition, patients reached equivalency to HCs in terms of unpleasantness while viewing SAD-related pictures (p < .02).
- 28. 3.2. Cross-lagged associations between emotion regulation and anxiety (Hypothesis 2) A summary of estimated cross-lagged fixed-effects are presented in Table 1. 3.2.1. Self-reported emotion regulation Frequency of suppression. Consistent with hypotheses, lower sup- pression frequency predicted lower subsequent clinician-rated (t81 = 2.11, p = .04, rs = .11 [.01, .29]) and self-reported anxiety (t86 = 2.41, p = .02, rs = .18 [.02, .35]). Thus, lower suppression frequency predicted lower anxiety four sessions later. Furthermore, neither clinician-rated (t81 = 1.46, p = .15, rs = .08 [.00, .26]) nor self- reported anxiety (t86 = 1.68, p = .10, rs = .08 [.00, .26]) predicted subsequent suppression frequency. These results suggest a unidirec- tional association whereby suppression frequency predicts subsequent anxiety and not the other way around. Frequency of reappraisal. In contrast to hypotheses, no significant cross-lagged associations were found between reappraisal frequency and anxiety (reappraisal→clinician-rated anxiety: t81 = -.39, p = .70,
- 29. rs = .02 [.00, .22]; reappraisal→self-reported anxiety: t86 = - .45, p = .65, rs = .02 [.00, .21]; clinician-rated anxiety → reappraisal: t81 = -.91, p = .37, rs = .07 [.00, .25]; self-reported anxiety → re- appraisal: t86 = -.55, p = .58, rs = .04 [.00, .22]). Self-efficacy of suppression. In partial support of hypotheses, greater suppression self-efficacy predicted lower subsequent self-re- ported (t86 = 2.25, p = .03, rs = .17 [.02, .34]) but not clinician- rated anxiety (t81 = 1.90, p = .06, rs = .09 [.00, .27]). In addition, neither clinician-rated (t81 = .97, p = .34, rs = .04 [.00, .23]) nor self- reported anxiety (t86 = 1.82, p = .07, rs = .07 [.00, .25]) predicted subsequent suppression self-efficacy. Self-efficacy of reappraisal. In partial support of hypotheses, greater reappraisal self-efficacy predicted lower subsequent self-re- ported (t86 = -2.09, p = .04, rs = .12 [.01, .30]) but not clinician-rated anxiety (t81 = -1.45, p = .15, rs = .06 [.00, .25]). Furthermore, in contrast to hypotheses, lower clinician-rated (t81 = 2.11, p = .04, rs = .11 [.01, .29]) and self-reported anxiety (t86 = -2.77, p < .01, rs = .11 [.01, .29]) predicted greater subsequent reappraisal self-effi- cacy. These results are more supportive of a unidirectional
- 30. relationship such that anxiety predicts subsequent reappraisal self-efficacy and not vice-versa.6 3.2. 2. Lab-based emotion regulation Unpleasantness ratings and electrocortical responses while viewing SAD-related pictures. Lower unpleasantness ratings while viewing SAD-related pictures predicted subsequent self-reported (t85 = - 2.50, p = .01, rs = .18 [.02, .35]), but not clinician-rated, anxiety (t80 = - 1.46, p = .15, rs = .09 [.00, .27]). However, lower clinician- rated (t80 = -2.39, p = .02, rs = .14 [.01, .32]) and lower self-reported an- xiety (t85 = -2.46, p = .02, rs = .14 [.01, .31]) predicted lower sub- sequent unpleasantness ratings. For electrocortical responses, smaller LPPs while viewing SAD- re- lated pictures predicted lower subsequent clinician-rated (t70 = 2.30, p = .02, rs = .12 [.01, .31]) and self-reported anxiety (t75 = 2.73, p < .01, rs = .17 [.01, .35]). In addition, anxiety did not predict subsequent LPPs while viewing SAD-related pictures (clinician-rated anxiety: b = -.02, t69 = -.36, p = .72, rs = .03 [.00, .24]; self-reported: t74 = -.72, p = .47, rs = .08 [.00, .27]). This suggests a unidirectional
- 31. association whereby lower electrocortical reactivity to SAD- related stimuli predicts lower anxiety four sessions later and not the other way around. Table 1 Estimated multi-level fixed effects and 95% confidence intervals for cross-lagged associations between emotion regulation and social anxiety. Emotion Regulation → Anxiety Anxiety → Emotion Regulation Emotion regulation variable Clinician-rated anxiety Self- reported anxiety Clinician-rated anxiety Self-reported anxiety ERQ Suppression frequency 2.92 [0.16, 5.67]* 2.34 [0.41, 4.28]* 0.01 [0.00, 0.02] 0.01 [0.00, 0.03] Reappraisal self-efficacy -2.55 [-6.05, 0.96] -2.46 [-4.80, - 0.12]* -0.01 [-0.02, 0.00]* -0.02 [-0.03, 0.00]** Suppression self-efficacy 2.72 [-0.12, 5.57] 2.49 [0.29, 4.69]* 0.00 [-0.01, 0.01] 0.01 [0.00, 0.03] Reappraisal frequency -0.62 [-3.80, 2.56] -0.44 [-2.38, 1.50] - 0.01 [-0.02, 0.01] -0.01 [-0.03, 0.01] Lab-based (ratings) View -4.22 [-9.96, 1.53] -4.41 [-7.92, -0.90]* -0.01 [-0.02, 0.00]* -0.01 [-0.02, 0.00]* Suppression -6.74 [-16.82, 3.35] 0.60 [-5.41, 6.61] 0.00 [0.00, 0.01] 0.00 [-0.01, 0.01] Reappraisal -0.30 [-5.77, 5.18] 1.99 [-1.00, 4.98] 0.01 [0.00, 0.01] 0.01 [0.00, 0.02] Lab-based (LPP) View 0.70 [0.09, 1.30]* 0.49 [0.13, 0.85]** -0.02 [-0.11, 0.08] - 0.06 [-0.21, 0.10] Suppression 0.28 [-0.25, 0.81] 0.00 [-0.32, 0.31] -0.04 [-0.13, 0.05] -0.03 [-0.15, 0.09]
- 32. Reappraisal -0.03 [-0.47, 0.42] 0.12 [-0.14, 0.38] 0.04 [-0.05, 0.13] -0.04 [-0.18, 0.10] Notes. ERQ = Emotion regulation questionnaire; LPP = Late positive potential. Clinician-rated and self-reported anxiety was measured using the Liebowitz Social Anxiety Scale and the Social Phobia Inventory, respectively. Lab-based reappraisal and suppression represent regulation change scores (view – regulate) with higher scores indicating larger regulation effects. */** significantly different from zero at p < .05/.01. 6 We also examined whether our findings are sensitive to the time lag between the measurement of emotion regulation and anxiety (one vs. four weeks) by refitting cross-lagged models of self-reported emotion regulation and self-re- ported anxiety with all weekly data. Lab-based emotion regulation and clin- ician-rated anxiety were only measured every four weeks and were not included in these analyses. We found that lower anxiety predicted lower subsequent suppression frequency and greater subsequent reappraisal self- efficacy, and not the other way around. The findings are reported in full in Supplemental Material, Section 5. Y. Kivity, et al. Journal of Affective Disorders 279 (2021) 334–342 339
- 33. Lab-based reappraisal and suppression. Reappraisal- and suppres- sion-related reductions in unpleasantness and electrocortical responses did not predict and were not predicted from clinician-rated and self- reported anxiety (ts = -1.33 – 1.88; ps = .06 – .98; rss = .00 – .12). 4. Discussion We utilized a multi-method design to examine the role of emotion regulation in CBT for SAD. CBT led to decreased self-reported frequency and self-efficacy of suppression, increased self-reported self- efficacy of reappraisal, decreased unpleasantness while viewing SAD- related pic- tures, and smaller reappraisal-related reductions in unpleasantness while viewing SAD-related pictures. Gains were maintained at 3- months follow-up. Lower suppression frequency and smaller electro- cortical reactivity predicted lower subsequent anxiety, but not vice versa. In contrast, self-efficacy of reappraisal and subjective reactivity to SAD-related pictures were predicted by previous levels of anxiety, but not vice versa. 4.1. Changes in emotion-regulation during treatment
- 34. Self-report findings are consistent with the literature regarding in- creases in reappraisal (Goldin et al., 2014a, 2017; Kocovski et al., 2013; Moscovitch et al., 2012), and partly consistent regarding decreases in suppression (Goldin et al., 2014a). Moscovitch et al. (2012) found no changes in suppression, which could be due to a number of reasons (e.g., different CBT protocols, insufficient power). Our study is novel in showing that patients reached normal levels of suppression, but not reappraisal. Thus, CBT seems to eliminate the initial overreliance on suppression among individuals with SAD – an impairment that has been shown to be large (e.g., g = 0.96 in Kivity & Huppert, 2019). Im- plementation of reappraisal seems to take more time to develop, pos- sibly due to its complexity. In terms of lab-based emotion regulation, we found decreased sub- jective reactivity to SAD-related pictures. Goldin et al. (2013) found similar reductions in reactivity that were specific to CBT compared with waitlist controls, and that only CBT patients reported an increase in automatic use of reappraisal during view. These findings, along with the finding that decreased subjective reactivity predicted lower sub-
- 35. sequent self-reported anxiety suggest that the reduction is unlikely to be due to practice effects (i.e., habituation due to the mere repeated ex- posure to the stimuli). Rather, it is possible that as treatment progresses, patients' automatic regulation increases even when passively viewing. This is consistent with our findings that the decrease in unpleasantness during reappraisal was mostly driven by reduction in unpleasantness while viewing pictures, and not by changes in unpleasantness in the reappraisal condition. It is noteworthy that floor effects could not be ruled out because unpleasantness was low at pre-treatment. However, even at post-treatment, unpleasantness while viewing SAD- related pictures did not reach the level of neutral pictures (see supplemental material, section 3, for descriptive statistics) making floor effect a less likely explanation. Finally, the LPP during lab-based regulation did not change, which is consistent with other studies reporting that the LPP is not larger among participants with social anxiety (Kivity & Huppert, 2018. 2019; Yuan et al., 2014, but see Kinney et al., 2019 for an exception). 4.2. The association between emotion-regulation and anxiety Lower frequency of suppression predicted lower subsequent
- 36. anxiety, but not the other way around. This supports a unidirectional association such that as patients make less attempts to hide their anxiety, their anxiety level decreases. This is consistent with the emphasis in CBT on reducing attempts to hide anxiety which is conveyed in several ways throughout treatment, such as in the psychoeducation module, outward shifting of attention (instead of on one's overt signs of anxiety) and in vivo exposures (patients are exposed to anxiety provoking situations while dropping safety behaviors that are intended to hide their an- xiety). Together with the finding that patients reached a normal level of suppression frequency, our findings point to a unique role of suppres- sion in CBT for SAD. Surprisingly, suppression did not predict subsequent anxiety in previous studies (Goldin et al., 2014a; Moscovitch et al., 2012). This divergence in findings could be due to the specific CBT protocol used in the current study that uniquely emphasizes outward shifting of atten- tion (Clark, 2005; Roth-Ledley et al., 2006). Our findings are consistent with a recent study showing that suppression, and not reappraisal, predicts subsequent anxiety in CBT for panic disorder (Strauss,
- 37. Kivity, & Huppert, 2019). In addition, in our sensitivity analyses, anxiety pre- dicted suppression in a one-week lag, but not vice versa. Thus, the exact time lag that determines the association between suppression and an- xiety needs to be further understood (c.f., Cole & Maxwell, 2003) and more studies examining the role of suppression in various CBT protocols are needed. Self-reported reappraisal did not reliably predict subsequent anxiety but rather was predicted by it. This is in contrast to previous studies showing that reappraisal predicted subsequent anxiety (Goldin et al., 2014a, 2017; Kocovski et al., 2015; Moscovitch et al., 2012). Together with our findings regarding suppression, it seems like the association between habitual emotion regulation and anxiety in CBT is dynamic, includes bidirectional influences between regulation and anxiety (c.f. Hofmann, Curtiss, & Hayes, 2020) and depends on the specific CBT protocol being used. Lower electrocortical reactivity to SAD-related stimuli predicted lower subsequent anxiety, but not vice versa. This unidirectional as- sociation was unique to electrocortical reactivity whereas
- 38. subjective reactivity seemed to be predicted by anxiety and not vice versa. Thus, while reductions in LPPs during treatment were not significant, they did predict outcome. This may suggest that some CBT patients become less reactive to SAD-related stimuli and that decreased reactivity is related to subsequent symptom reduction. The mechanism underlying this re- duction remains to be examined. For example, the decreased reactivity could be related to use of automatic reappraisal (that is not captured by the lab-based task) or to improvements in other regulation strategies that are known to be impaired in SAD such as rumination (Kashdan & Roberts, 2007) and avoidance (Heur, Rinck, & Becker, 2007). Other than the abovementioned findings, lab-based regulation did not improve and was unrelated to outcome. This is consistent with the lack of impairments in social anxiety compared to controls in lab-based tasks (Gaebler et al., 2014; Goldin et al., 2009b; Kinney et al., 2019; Kivity & Huppert, 2018, 2019; Yuan et al., 2014; but see Ziv, Goldin, Jazaieri, Hahn, & Gross, 2013 for a significant finding in one out of three tasks). Along with daily diaries studies showing impaired emotion regulation (e.g., Kivity & Huppert, 2016), our findings suggest
- 39. that individuals with SAD are able to regulate upon instruction, but have difficulties implementing their abilities in daily life. However, one study found specific CBT-related decreases in emotion intensity ratings and modulation of fMRI activity during reappraisal of negative social evaluations (Goldin et al., 2013, 2014b). These differences could either stem from the different tasks used, the measure of brain activity (ERPs vs. fMRI), or the materials used (standardized pictures vs. idiographic self-referential social evaluations). Taken together, our findings suggest that CBT eliminates the over- reliance on suppression and that this reduction in suppression fre- quency plays an important role in CBT for SAD whereas reappraisal does not. This is only partly consistent with the Heimberg model (Morrison & Heimberg, 2013) which attributes a role to both suppres- sion and reappraisal in CBT for SAD. Thus, as more findings accrue, the model could be modified to put a larger emphasis on suppression re- lative to reappraisal. Furthermore, models should explicitly articulate the ways in which CBT is hypothesized to reduce suppression (e.g., outward shifting of attention, dropping safety behaviors). Future
- 40. Y. Kivity, et al. Journal of Affective Disorders 279 (2021) 334–342 340 studies could empirically examine these propositions and potentially improve existing protocols. Finally, at least one other route for anxiety reduction exist in CBT that occurs through diminished reactivity to SAD-related stimuli. This remains to be further understood in future studies. 5. Limitations Despite the multiple assessment points, our sample was moderate in size. Relatedly, unbiased crossed-lagged estimates an accurate time lag between cause and outcome (Cole & Maxwell, 2003). Such information is available for emotion regulation-social anxiety associations, and we mostly focused on four-weeks lags. Additional studies with intensive measurements are needed to determine the most accurate time lags. Finally, without a treatment control group, it is difficult to rule out that the observed changes were not due to the mere passage of time. However, the finding that changes in emotion regulation were
- 41. only observed during treatment but not from post-treatment to follow-up reduce the likelihood of changes due to the passage of time only. Still, the lack of a control group makes it impossible to determine the spe- cificity of the findings to CBT compared to other treatments. 6. Conclusions CBT for SAD reduced emotion dysregulation as revealed by self- reports and subjective emotional reactivity. Most notably, patients reached a normal level of suppression frequency. In addition, sup- pression frequency and electrocortical reactivity emerged as unidirec- tional predictors of subsequent anxiety while the role of other types of emotion regulation was less clear. This suggests that emotion regula- tion, and especially suppression, may play a complex, causal role in CBT for SAD. If these findings are replicated, they might have important theore- tical and clinical implications for models of CBT for SAD. Models and protocols may need to assign a greater role to suppression and a lesser role to reappraisal. Our study also highlights the importance of multi- method designs when examining emotion regulation during
- 42. treatment while specifying the exact nature of emotion dysregulation and focusing on the possible difficulties in implementing otherwise intact regulation abilities in daily life. Author Contributions Y.K. developed the concept, performed the data analysis and in- terpretation and drafted the paper for the current report under the supervision of J.D.H. J.D.H developed the overall study concept and design. All authors contributed to data collection, provided critical re- visions and approved the final manuscript for submission. Declaration of Competing Interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influ- ence the work reported in this paper. Acknowledgements The authors would like to thank Roni Pener-Tessler, Ariela Friedman, Asher Strauss, Yael Milgram, Shai Avishay, Michal Kovacs, and Maayan Langmass for their help in data collection and Jason Moser and members of the clinical psychophysiology lab for their help in analyses of the ERP data. Preparation of this manuscript was
- 43. supported by a grant from the Israel Science Foundation (grant #332/09) to the last author, the Sam and Helen Beber Chair of Clinical Psychology at The Hebrew University. The funding sources did not have any in- volvement in conducting the study and preparing the manuscript. Supplementary materials Supplementary material associated with this article can be found, in the online version, at doi:10.1016/j.jad.2020.10.021. References American Psychiatric Association (2000). Diagnostic and statistical manual of mental dis- orders (4th ed., text rev. ed.). Washington, DC: Author. Carthy, T., Horesh, N., Apter, A., Edge, M.D., Gross, J.J., 2010. Emotional reactivity and cognitive regulation in anxious children. Behaviour Research and Therapy 5 (48), 384–393. Clark, D.M., 2005. A cognitive perspective on social phobia. In: Crozier, W.R., Alden, L.E. (Eds.), The Essential Handbook of Social Anxiety for Clinicians. Wiley, Chichester, pp. 193–218. Cole, D., Maxwell, S., 2003. Testing mediational models with
- 44. longitudinal data: questions and tips in the use of structural equation modeling. Journal of Abnormal Psychology 112 (4), 558–577. Connor, K.M., Davidson, J.R., Churchill, L.E., Sherwood, A., Weisler, R.H., Foa, E., 2000. Psychometric properties of the Social Phobia Inventory (SPIN): New self-rating scale. The British Journal of Psychiatry 176 (4), 379–386. Dryman, M.T., Heimberg, R.G., 2018. Emotion regulation in social anxiety and depres- sion: a systematic review of expressive suppression and cognitive reappraisal. Clinical Psychology Review 65, 17–42. Falkenström, F., Finkel, S., Sandell, R., Rubel, J.A., Holmqvist, R., 2017. Dynamic models of individual change in psychotherapy process research. Journal of Consulting and Clinical Psychology 85 (6), 537–549. Farmer, A.S., Kashdan, T.B., 2012. Social anxiety and emotion regulation in daily life: Spillover effects on positive and negative social events. Cognitive Behaviour Therapy 41 (2), 152–162. Foti, D., Hajcak, G., 2008. Deconstructing reappraisal: Descriptions preceding arousing pictures modulate the subsequent neural response. Journal of Cognitive Neuroscience 20 (6), 977–988. Gaebler, M., Daniels, J.K., Lamke, J.-P., Fydrich, T., Walter,
- 45. H., 2014. Behavioural and neural correlates of self-focused emotion regulation in social anxiety disorder. Journal of Psychiatry & Neuroscience 39 (4), 249–258. Goldin, P.R., Lee, I., Ziv, M., Jazaieri, H., Heimberg, R.G., Gross, J.J., 2014a. Trajectories of change in emotion regulation and social anxiety during Cognitive Behavioral therapy for social anxiety disorder. Behaviour Research and Therapy 56, 7–15. Goldin, P.R., Manber, T., Hakimi, S., Canli, T., Gross, J.J., 2009a. Neural bases of social anxiety disorder: emotional reactivity and cognitive regulation during social and physical threat. Archives of General Psychiatry 66 (2), 170– 180. Goldin, P.R., Manber-Ball, T., Werner, K., Heimberg, R., Gross, J.J., 2009b. Neural me- chanisms of cognitive reappraisal of negative self-beliefs in social anxiety disorder. Biological Psychiatry 66 (12), 1091–1099. Goldin, P.R., Morrison, A.S., Jazaieri, H., Heimberg, R.G., Gross, J.J., 2017. Trajectories of social anxiety, cognitive reappraisal, and mindfulness during an RCT of CBGT versus MBSR for social anxiety disorder. Behaviour Research and Therapy 97, 1–13. Goldin, P.R., Ziv, M., Jazaieri, H., Hahn, K., Heimberg, R., Gross, J.J., 2013. Impact of cognitive behavioral therapy for social anxiety disorder on the neural dynamics of
- 46. cognitive reappraisal of negative self-beliefs: randomized clinical trial. JAMA Psychiatry 70 (10), 1048–1056. Goldin, P.R., Ziv, M., Jazaieri, H., Weeks, J., Heimberg, R.G., Gross, J.J., 2014b. Impact of Cognitive Behavioral therapy for social anxiety disorder on the neural bases of emotional reactivity to and regulation of social evaluation. Behaviour Research and Therapy 62, 97–106. Gross, J., John, O., 2003. Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. Journal of personality and so- cial psychology 85 (2), 348–362. Gross, J.J., 2015. Emotion regulation: Current status and future prospects. Psychological Inquiry 26 (1), 1–26. Hajcak, G., Nieuwenhuis, S., 2006. Reappraisal modulates the electrocortical response to unpleasant pictures. Cognitive, Affective, & Behavioral Neuroscience 6 (4), 291–297. Heuer, K., Rinck, M., Becker, E.S., 2007. Avoidance of emotional facial expressions in social anxiety: The approach–avoidance task. Behaviour Research and Therapy 45 (12), 2990–3001. Hofmann, S.G., Curtiss, J.E., Hayes, S.C., 2020. Beyond linear mediation: Toward a dy- namic network approach to study treatment processes. Clinical
- 47. Psychology Review 76. Hofmann, S.G., Sawyer, A.T., Fang, A., Asnaani, A., 2012. Emotion dysregulation model of mood and anxiety disorders. Depression and Anxiety 29 (5), 409–416. Huppert, J.D., Kivity, Y., Cohen, L., Strauss, A., Elizur, Y., Weiss, M., 2018. A pilot ran- domized clinical trial of cognitive behavioral therapy versus attentional bias mod- ification for social anxiety disorder: An examination of outcomes and theory-based mechanisms. Journal of Anxiety Disorders 59, 1–9. Jaeger, B.C., Edwards, L.J., Das, K., Sen, P.K., 2016. An R 2 statistic for fixed effects in the Y. Kivity, et al. Journal of Affective Disorders 279 (2021) 334–342 341 https://doi.org/10.1016/j.jad.2020.10.021 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0002 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0002 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0002 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0003 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0003 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0003 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0004 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0004 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0004 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0005 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0005
- 49. http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0020 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0020 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0020 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0021 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0021 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0022 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0022 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0023 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0023 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0023 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0024 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0024 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0024 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0025 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0025 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0026 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0026 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0026 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0026 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0027 generalized linear mixed model. Journal of Applied Statistics 44 (6), 1086–1105. Jaeger, B. C., & R Core Team. (2016). r2glmm: R Squared for Mixed (Multilevel) Models, R package version 0.1.1 [Computer software]. Retrieved from https://github.com/ bcjaeger/r2glmm. Kashdan, T.B., Roberts, J.E., 2007. Social anxiety, depressive symptoms, and post-event rumination: Affective consequences and social contextual influences. Journal of Anxiety Disorders 21 (3), 284–301.
- 50. Kendall, P., Marrs-Garcia, A., Nath, S., Sheldrick, R., 1999. Normative comparisons for the evaluation of clinical significance. Journal of Consulting and Clinical Psychology 67 (3), 285–299. Kinney, K.L., Burkhouse, K.L., Klumpp, H., 2019. Self-report and neurophysiological in- dicators of emotion processing and regulation in social anxiety disorder. Biological Psychology, 142 126–131. Kivity, Y., Huppert, J.D., 2018. Are individuals with social anxiety successful in reg- ulating their emotions? A mixed-method investigation using self-report, behavioral, and event-related potentials measures. Journal of Affective Disorders 236, 298–305. Kivity, Y., Huppert, J.D., 2019. Emotion regulation in social anxiety: A systematic in- vestigation using self-report, behavioral, and event-related potentials measures. Cognition & Emotion 33, 213–230. Kivity, Y., Huppert, J.D., 2016. Does cognitive reappraisal reduce anxiety? A daily diary study of a micro-intervention with individuals with high social anxiety. Journal of Consulting and Clinical Psychology 84 (3), 269–283. Kocovski, N.L., Fleming, J.E., Hawley, L.L., Ho, M.-H.R., Antony, M.M., 2015. Mindfulness and acceptance-based group therapy and traditional cognitive beha-
- 51. vioral group therapy for social anxiety disorder: Mechanisms of change. Behaviour Research and Therapy 70, 11–22. Kocovski, N.L., Fleming, J.E., Hawley, L.L., Huta, V., Antony, M.M., 2013. Mindfulness and acceptance-based group therapy versus traditional cognitive behavioral group therapy for social anxiety disorder: A randomized controlled trial. Behaviour Research and Therapy 12 (51), 889–898. Lang, P.J., Bradley, M.M., Cuthbert, B.N., 2008. International affective picture system (IAPS): Affective ratings of pictures and instruction manual. University of Florida, Gainesville, FL. Levin, J.B., Marom, S., Gur, S., Wechter, D., Hermesh, H., 2002. Psychometric properties and three proposed subscales of a self-report version of the Liebowitz Social Anxiety Scale translated into Hebrew. Depression and Anxiety 16 (4), 143–151. Liebowitz, M.R., 1987. Social phobia. Modern problems of Pharmacopsychiatry 22, 141–173. Moran, T.P., Jendrusina, A.A., Moser, J.S., 2013. The psychometric properties of the late positive potential during emotion processing and regulation. Brain Research 1516, 66–75.
- 52. Morrison, A.S., Heimberg, R.G., 2013. Social anxiety and social anxiety disorder. Annual Review of Clinical Psychology 9, 249–274. Moscovitch, D.A., 2009. What is the core fear in social phobia? A new model to facilitate individualized case conceptualization and treatment. Cognitive and Behavioral Practice 16, 123–134. Moscovitch, D.A., Gavric, D.L., Senn, J.M., Santesso, D.L., Miskovic, V., Schmidt, L.A., Antony, M.M., 2012. Changes in judgment biases and use of emotion regulation strategies during Cognitive Behavioral therapy for social anxiety disorder: Distinguishing treatment responders from nonresponders. Cognitive Therapy and Research 36 (4), 261–271. Moser, J.S., Hartwig, R., Moran, T.P., Jendrusina, A.A., Kross, E., 2014. Neural markers of positive reappraisal and their associations with trait reappraisal and worry. Journal of Abnormal Psychology 123 (1), 91–105. Nock, M.K., 2007. Conceptual and design essentials for evaluating mechanisms of change. Alcoholism: Clinical and Experimental Research 31 (S3), 4S– 12S. Pinheiro, J., Bates, D., DebRoy, S., Sarkar, D., & R Core Team. (2016). nlme: Linear and Nonlinear Mixed Effects Models, R package version 3.1-128 [Computer software]. Retrieved from http://CRAN.R-project.org/package=nlme.
- 53. Proudfit, G.H., Dunning, J., Foti, D., Weinberg, A., 2013. Temporal dynamics of emotion regulation. In: Gross, J.J. (Ed.), Handbook of Emotion Regulation, 2nd ed. Guilford Publications, New York, pp. 43–57. Roth-Ledley, D.A., Foa, E.B., Huppert, J.D., 2006. Comprehensive Cognitive Behavior Therapy for Social Phobia: A Treatment Manual. University of Pennsylvania, Philadelphia, PA. Sheehan, D.V., Lecrubier, Y., Sheehan, K.H., Amorim, P., Janavs, J., Weiller, E., Dunbar, G.C., 1998. The Mini-International Neuropsychiatric Interview (MINI): The devel- opment and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. Journal of Clinical Psychiatry 59, 22–33. Strauss, A.Y., Kivity, Y., Huppert, J.D., 2019. Emotion Regulation Strategies in Cognitive Behavioral Therapy for Panic Disorder. Behavior Therapy 50, 659–671. Wang, L., Maxwell, S., 2015. On disaggregating between- person and within-person effects with longitudinal data using multilevel models. Psychological Methods 20 (1), 63–83. Yuan, L., Zhou, R., Hu, S., 2014. Cognitive reappraisal of facial expressions: Electrophysiological evidence of social anxiety. Neuroscience Letters 577, 45–50.
- 54. Ziv, M., Goldin, P.R., Jazaieri, H., Hahn, K.S., Gross, J.J., 2013. Emotion regulation in social anxiety disorder: behavioral and neural responses to three socio-emotional tasks. Biology of Mood & Anxiety Disorders 3 (1), 20–36. Y. Kivity, et al. Journal of Affective Disorders 279 (2021) 334–342 342 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0027 https://github.com/bcjaeger/r2glmm https://github.com/bcjaeger/r2glmm http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0029 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0029 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0029 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0030 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0030 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0030 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0031 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0031 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0031 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0032 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0032 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0032 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0033 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0033 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0033 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0034 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0034 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0034 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0036 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0036 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0036 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0036
- 56. http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0049 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0050 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0050 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0050 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0050 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0051 http://refhub.elsevi er.com/S0165-0327(20)32865-2/sbref0051 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0052 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0052 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0053 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0053 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0054 http://refhub.elsevier.com/S0165-0327(20)32865-2/sbref0054 http://refhub.elsevier.com/S0165-0327(20)32865- 2/sbref0054The role of expressive suppression and cognitive reappraisal in cognitive behavioral therapy for social anxiety disorder: A study of self-report, subjective, and electrocortical measures1 Introduction2 Method2.1 Participants2.2 Measures2.3 Treatment and therapists2.4 Procedure2.5 Data Analyses3 Results3.1 Changes in regulation (H1) and equivalency to HCs (H3)3.1.1 Change in self-reports3.1.2 Change in lab-based measures3.1.3 Equivalency to HCs3.2 Cross-lagged associations between emotion regulation and anxiety (Hypothesis 2)3.2.1 Self-reported emotion regulation3.2 2. Lab-based emotion regulation4 Discussion4.1 Changes in emotion-regulation during treatment4.2 The association between emotion-regulation and anxiety5 Limitations6 ConclusionsAuthor ContributionsDeclaration of Competing InterestAcknowledgementsSupplementary materialsReferences
- 57. Cultural Aspects of Social Anxiety Disorder: A Qualitative Analysis of Anxiety Experiences and Interpretation Abolafzl Mohammadi 1 , Imaneh Abasi 2 *, Mehdi Soleimani 1 , Seyed Tayeb Moradian 3 , Taha Yahyavi 4 , Mostafa Zarean 5 Abstract Objective: Anxiety is a complex phenomenon on which culture has a prominent influence. The present study aimed to investigate the cultural aspects of social anxiety disorder (SAD) in an Iranian population. Method: A qualitative content analysis research was done to
- 58. answer the study question. A total of 16 individuals with social anxiety disorder (six men and 10 women) were selected using purposeful sampling method (M = 24.43, SD = 4.56). The study was conducted in Tehran, Urmia, and Sanandaj- Iran. Participants were from different ethnic backgrounds (LOR, FARS, TURK, and KURD). Data were analyzed by thematic analysis using an inductive method. Results: Analysis of participants’ records yielded five distinct categories with some subcategories, which are as follow: (1) anxiety experiences; (2) core beliefs; (3) reasons of being anxious; (4) effects of SAD on life aspects; and (5) coping strategies. Conclusion: It seems that symptoms of social anxiety and its underlying beliefs, causes and effects and coping strategies are almost experienced and interpreted in a way that could be the same as DSM-5 clinical presentation of social anxiety, with the exception that somatic symptoms are experienced by almost all participants. Key words: Anxiety; Culture; Qualitative Research; Social Anxiety Disorder Anxiety disorders are the most prevalent psychiatric disorders (1). They affect various aspects of life, including social, financial, educational, relationship, and quality of life. Anxiety disorders are the result of genetic, environmental, familial, mental, and cultural
- 59. factors (2, 3). Anxiety disorders are affected by cultural features (4, 5); and symptoms and variation in prevalence of anxiety disorders could be transformed across ethnicities and cultures (6, 7). Cultural values and beliefs may put individuals at risk and they may also act as a buffer against anxiety problems (8). Culture plays an important role in awareness toward problem severity and its consequences and health care searching behaviors (9). In line with cultural influences on anxiety disorders, a review showed that unexpectedness and 10-minute
- 60. crescendo criteria in panic disorder, definition of social anxiety and social reference group in social anxiety disorder, and the preference given to psychological symptoms of worry in generalized anxiety disorder are phenomenological expressions in different cultures (10). Individualism vs. collectivism nature of countries may be related to social anxiety differently (11). Furthermore, khyâl cap (wind attacks), taijin kyofusho, and ataques de nervios are three main examples of culture-specific expressions of anxiety disorders, which have been included in DSM-V as distress concepts (12). Iran J Psychiatry 2019; 14: 1: 33-39
- 61. Original Article 1. Department of Psychiatry, School of Medicine, Tehran University of Medical Sciences, Tehran, Iran. 2. Department of Clinical Psychology, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. 3. Atherosclerosis Research Center, Baqiyatallah University of Medical Sciences, Tehran, Iran. 4. Department of Psychiatry, School of Medicine, Tehran University of Medical Sciences, Tehran, Iran. 5. Department of Psychology, School of Education and Psychology, Tabriz University, Tabriz, Iran. *Corresponding Author: Address: Department of Clinical Psychology, University of Social Welfare and Rehabilitation Sciences, kodakyar Avenue, Daneshjo Boulevard, Evin, Tehran, Iran. Postal Code: 1985713834 Tel: 98-2122180045, Fax: 98-2122180045, Email: [email protected] Article Information: Received Date: 2018/04/11, Revised Date: 2018/08/18, Accepted Date: 2018/09/16
- 62. Mohammadi, Abasi, Soleimani, et al. Iranian J Psychiatry 14: 1, January 2019 ijps.tums.ac.ir 34 A study on anxiety and its cultural complexities in Iran showed that individuals with Azeri ethnicity (one of several Iranian ethnicities) suffering from emotional disorders reported 11 main themes as avoidance, dysfunction, arousal, disorganized personality, repetition, somatization, problematic behavior, maladaptive cognition, awareness, and positive and negative emotionality, among which somatization had the highest frequency (13). There is strong evidence that individuals from non-Western cultures significantly report more somatic rather than psychological symptoms (14, 15). In this study, we used the term culture and ethnicity interchangeably to refer to common heritage, shared beliefs, and norms of a unit or a group of people. Iran is
- 63. a country with different cultural and ethnical background, and this may be responsible for various psychological manifestations. Moreover, there is no adequate information about cultural aspects of anxiety in Iranian population and because of the prominence of cultural effects on anxiety symptoms (8, 9 and 12) and culture-gene interactions (16, 17), studying the cultural nature of anxiety disorders in Iranian population is of utmost importance. Furthermore, the anxiety phenomenon is extremely complex and passing of time makes it even more complex in some ways, so the best way to clarify a content-based phenomenon is to conduct a qualitative research. The qualitative method can illuminate some phenomena which could not be reached out through qualitative methods. Moreover, it can also help understand different perspectives and contribute to mental health policy (18) . The main objective of this research was to study the
- 64. cultural aspects of anxiety, mainly social anxiety, in four ethnic groups (LOR, FARS, TURK, and KURD) in Iran, who were diagnosed with social anxiety disorder. Thus, generalization is possible. Specific aims in this research were as follow: describing anxiety experience among people suffering from anxiety disorders; evaluating awareness and experience of anxiety among general people; determining the causes of perceived anxiety among participants in the study; describing the participants’ opinions towards prognoses and consequences of anxiety, describing the participants’ opinions towards prevention and treatment of anxiety disorders. Materials and Methods The study design is a qualitative content analysis research. Study conducted in the cities of Tehran, Urmia, and Sanandaj- Iran. A total of 16 individuals with social anxiety disorders (six men and 10 women) were selected
- 65. via purposeful sampling method (M = 24.43, SD = 4.56). With respect to education level, nine participants had high school diploma, one had a bachelor’s degree, and six had a master’s degree. With respect to ethnicity, one participant was identified as Lor, two as Fars, six as Turk, and seven as Kurd. Patients were selected according to some inclusion and exclusion criteria and were recruited from counseling centers in aforementioned cities. Main inclusion criteria were age>18 and primary diagnosis of social anxiety disorder. Main exclusion criteria were as follow: comorbid with any debilitating mental illness like schizophrenia, bipolar disorder, substance abuse, and mental retardation; comorbid with debilitating physical illness. The study was done during 2016-2017. All individuals were interviewed by a psychiatrist and were diagnosed as social anxiety disorder. Then, they were informed about the purpose of study, and informed consent was
- 66. obtained from all of them. All voluntary participants were asked open ended questions by a clinical psychologist (MS.c.) through an in-depth and semi- structured interview. Answers were audio recorded and lasted 30 to 60 minutes. Questions were categorized into three main groups: (1) personal experiences and perception about anxiety; (2) factors causing anxiety; and (3) coping strategies when feeling anxious. Ethical approval was obtained from the National Institute for Medical Research Development. Informed consent was obtained before interviewing. Participants were assured about the confidentiality of their information and were debriefed about the purpose of the study . Analysis Results of the interview with each participant were recorded, coded, and categorized. Overall, the interviewed data were processed through thematic analysis. An inductive method was used for data analysis
- 67. (19). Results Participants’ description of their experiences and beliefs about coping consequences of anxiety, SAD reasons, and coping strategies when facing anxiety were categorized in the following categories (Table 1). 1 .Symptoms of Anxiety 1.1 Emotional Anxiety was experienced mainly in public (feeling anxious when speaking, asking questions, and commenting) and in classroom (anxiety when presenting, providing training courses, asking questions, speaking, and commenting). Example Participant 1: I am afraid of speaking in public because I feel I am not good at it . 1.2 .Cognitive
- 68. Cognitive aspect of anxiety was categorized into two main categories as pre event rumination (thinking of making a mistake and thinking of being humiliated, thinking of being mocked, and thinking of not being able to handle the situation) and post event rumination (thinking of making mistakes, thinking of being humiliated, and thinking of being mocked). Example Cultural Aspects of Social Anxiety Disorder Iranian J Psychiatry 14: 1, January 2019 ijps.tums.ac.ir 35 Participant 2. I am afraid of making mistakes and classmates laugh at me because of it. 1.3 Behavioral Behavioral aspect was categorized into 3 main sections as avoidance (avoiding stressful situations), surrender (inability of movement and inability to speak), and safety behaviors (talking fast).
- 69. Example Participant 5: When I am in stressful situations I can’t speak or move, it is like I am in a cage . 1.4 Physical Physical aspect consisted of several symptoms including increasing heartbeat, feeling cold, feeling pressure on the head, sweating, hoarseness, inability to swallow saliva, suffocation, body weakness, lowering the pressure of the body, blushing, feeling hot in the body, difficulty sleeping, feeling of losing balance, flushing, and lowering the tone of voice . Example Participant 9: when I am anxious, I feel flushed, I feel I am losing balance, and I feel hot in my body. 2 .Core Beliefs Profound beliefs related to social anxiety experienced by participants were categorized in following categories:
- 70. 2.1 Fear of negative evaluation: Being neglected by others, rejected, mocked by others, loss of pride, loss of popularity, and feeling ashamed. Example Participant 10: When I want to give presentation in class, I feel like everybody is looking at me, they are making fun of me, and they think I am not good at it . 2.2 Unworthiness: Not being worthy, not being satisfied with oneself . Example Participant 12: I think something makes me most vulnerable in these situations and that is I don’t feel worthy enough. 2.3 Incompetency: loss, failure. Example Participant 7: When I think of my SAD symptoms, I think about my previous failures. 3 .Reasons of Being Anxious
- 71. 3.1 Familial factors: Family tension, parental punishment, parental harshness, incorrect parenting systems, and emotional deprivation. Example Participant 13: I was raised in a family full of tension and stress that were beyond my ability to manage . 3.2 Fear: Fear of negative evaluation, fear of being rejected, and losing loved ones . Example Participant 13: I think fear of other`s views about us and fear of being rejected by them can make us anxious. 3.3 Core beliefs: Unworthiness and incompetency. Example Participant 16: In an anxious situation, I really feel like I can’t help myself and this may be the reason of my anxiety. 3.3 Society: Poverty and school (poor education and inappropriate laws).
- 72. Example Participant 15: I have been faced with poverty and other stresses several times and since then I have been so tensed and anxious. 4 .Effects of SAD on Life Aspects 4.1 .Social dysfunction (inability to speak in front of others, inability to connect with others, inability to make friends, inability to go out alone, losing job opportunities, avoiding social relationships, and failure to establish a relationship with the opposite sex). 4.2 .Emotional dysfunction (worry, lowering fear threshold, and feeling disappointed) Example Participant 14: Social anxiety has ruined my life. I am always worried about social situations . 4.3 .Behavioral Dysfunction (poor quality of life, avoiding stressful situations)
- 73. Example Participant 11: I don’t take part in social situations where I am not acquainted. 5 .Coping Mechanisms Participant’s explanation about strategies for handling their anxiety was categorized in following sections: 5.1 .Treatment (psychotherapy and pharmacotherapy) Example Participant 12: A psychologist or a psychiatrist may be helpful . 5.2 .Emotion-based mechanisms (watching movies, overeating, sleeping, avoiding stressful situations, praying, talking to others, drinking, smoking, listening to music, and relaxing) Example Participant 11: When I am worried or anxious, I eat and sometimes I listen to music. 5.3 .Problem-based strategies (studying psychological
- 74. books, practicing for presentation or speaking, studying more about the presentation subject). Example Participant 8: I analyze the situation and find some logical solutions for it, but it doesn’t always work . 5.4 .Behavioral and Cognitive Strategies (positive self- statements, distractions, and avoiding eye contact). Example Participant 5: In classroom, when I am talking about something, I cannot look in the eyes of others . Furthermore, when participants were asked about the onset of their social anxiety symptoms, some of them stated that they had these feelings since childhood and most of them pointed to some events, such as a new job/changing job, teachers, and inappropriate behavior.
- 75. Mohammadi, Abasi, Soleimani, et al. Iranian J Psychiatry 14: 1, January 2019 ijps.tums.ac.ir 36 Table 1. Participants’ Categories of Experienced Social Anxiety Symptoms Presented as Main Categories, Subcategories, and Meaningful Codes Categories Subcategories Codes Anxiety experiences Emotional (public and classroom) Feeling anxious when speaking Asking questions Commenting Providing training courses Cognitive (pre event rumination, and post event rumination) Thinking of making mistakes Thinking of being humiliated Thinking of being mocked
- 76. Thinking of not being able to handle the situation Behavioral (avoidance, surrender, and safety behaviors) Avoiding stressful situations Inability to move and inability to speak Talking fast Physical Increasing heartbeat Feeling cold in the body Feeling pressure on the head Sweating Hoarseness Inability to swallow saliva Suffocation Body weakness Lowering the pressure of the body Blushing Feeling hot in the body
- 77. Difficulty sleeping Feeling losing balance Flushing Lowering the tone of voice Core beliefs Fear of negative evaluation Being neglected by others Being rejected Bg mocked by others Loss of pride Loss of popularity Feeling ashamed in front of others The negative thoughts of others about oneself Unworthiness Not being worthy Not being satisfied with oneself Incompetency Loss, failure Reasons of being anxious Familial factors
- 78. Family tension Parental punishment Parental harshness Incorrect parenting systems Emotional deprivation Fear Fear of negative evaluation Fear of being rejected Fear of losing important others Core Beliefs Unworthiness and incompetency Society Poverty and school Cultural Aspects of Social Anxiety Disorder Iranian J Psychiatry 14: 1, January 2019 ijps.tums.ac.ir 37 Effects of SAD on life aspects Social dysfunction
- 79. Inability to speak in front of others, inability to connect with others, inability to make friends, inability to go out alone, losing job opportunities, avoiding social relationships, little to say, and failure to establish a relationship with the opposite sex Emotional dysfunction Worry Lowering fear threshold Feeling disappointed Behavioral dysfunction Poor quality of life, avoiding stressful situations Coping mechanisms Treatment Psychotherapy Pharmacotherapy Emotion-based mechanisms Watching movies Overeating, sleeping
- 80. Avoiding stressful situations Praying Talking with others Drinking Smoking Listening to music Relaxation Problem-based mechanisms Studying psychological books to practice for presentation or speaking Studying more about the presentation subject Behavioral and Cognitive strategies Positive self-statements Distractions Avoiding eye contact Discussion The present research was a qualitative study on anxiety experiences and responses to anxiety among individuals
- 81. suffering from social anxiety disorder. This was the first study in Iran to investigate some questions surrounding the underlying experiences of anxiety and coping strategies toward anxiety. Analysis of participants’ records yielded five distinct themes: (1) anxiety experiences; (2) core beliefs; (3) reasons of being anxious; (4) effects of SAD on life aspects; and (5) coping strategies . Anxiety symptoms reported by participants in this study are similar to the last DSM criteria on SAD symptoms showing that these symptoms are being experienced globally (20). Moreover, these findings are comparable with previous studies showing that there are no significant differences between Americans and Japanese on SAD symptoms; however, Taijin Kyofusho, which is a form of social anxiety in Japanese culture, was more reported by Japanese individuals (21), indicating that some form of SAD may be more culturally dependent
- 82. and treatment should be tailored for them. Physical symptoms, not a main symptom of SAD, were reported significantly and by most participants of the present study. This finding is consistent with that of previous studies demonstrating this notion that people in non-Western or Eastern countries (9), including Iran (22), tend to somatize their distress and anxiety because of different ethnomedical beliefs about physical symptoms (23) or because they have learned to somatize their distress to get more attention . Results of core beliefs showed 3 main subthemes as fear of negative evaluation, unworthiness, and inadequacy. Fear of negative evaluation is the defining feature and core of social anxiety (20). Unworthiness and inadequacy are two underlying cognitions in classical cognitive theory that predispose individuals to interpret stimuli in a distorted way and as a result experience
- 83. social anxiety symptoms (24). In case of causes of SAD, participants attribute SAD to psychological (fear and core beliefs) and non- psychological (society and family) processes; and the impact of non-psychological process was highlighted. This is in line with a previous study (25) and indicate that Iran as a developing country with a different culture and various ethnicities is exposed to many social, economic, and political deprivations, which affect Iranians’ life in unpleasant ways . Mohammadi, Abasi, Soleimani, et al. Iranian J Psychiatry 14: 1, January 2019 ijps.tums.ac.ir 38 Analysis of data revealed that social anxiety symptoms affect individuals’ life in various ways (social, emotional, and behavioral), and this supports previous studies indicating low quality of life in the participants (26).
- 84. With respect to coping strategies, four main themes (treatment, emotion-based mechanisms, problem-based mechanisms, and behavioral and cognitive strategies) were reported. Among them, praying and a special bond with God were significantly reported. This finding showed that Iran is a religious country and spirituali ty could make a bigger difference in people’s lives and it is used willingly by individuals with SAD as one of main coping strategies. Inconsistent with this result, previous studies have indicated the contributory role of religion and spirituality in SAD (27). Limitation This study was the first in its field of inquiry. However, there were some limitations that should be considered carefully. First, this was a qualitative study and thus findings should be generalized to other SAD individuals with caution. Second, although in the present study participants were from different ethnicities, the
- 85. difference between ethnicities in experiencing anxiety and its related factors was not investigated. Thus, future studies should be conducted to take a deeper look into this topic. Third, there are some transdiagnostic and common factors between disorders, especially emotional disorders, which play an important role in etiology and treatment of emotional disorders. Finally, the present study assessed only four ethnicities and did not include others. Conclusion The present study highlighted the importance of experiencing social anxiety, interpretation of causes of social anxiety, underlying beliefs of SAD and its effects, and coping strategies in the diverse ethnic population of Iran. Moreover, this study was the first of its kind, especially in Iran, as a Middle-Eastern country. Findings of the present study indicated that SAD symptoms and the related psychological processes are a global problem
- 86. and this could be due to social media and other mass media making people around the world more and more alike. Acknowledgment We thank all participants of the present study. Conflict of Interest The authors have confirmed that there are not any conflicts of interest. References 1. Remes O, Brayne C, Linde R, Lafortune L. A systematic review of reviews on the prevalence of anxiety disorders in adult populations. Brain Behav. 2016;6:e00497. 2. Essau CA, Conradt J, Petermann F. Frequency, comorbidity, and psychosocial impairment of anxiety disorders in German adolescents. J Anxiety Disord. 2000;14(3):263-79. 3. McLean CP, Asnaani A, Litz BT, Hofmann SG. Gender differences in anxiety disorders: prevalence, course of illness, comorbidity and burden of illness. J Psychiatr Res.
- 87. 2011;45(8):1027-35. 4. Stein DJ, Williams D. Cultural and social aspects of anxiety disorders. Textbook of Anxiety Disorders Washington, DC: American Psychiatric Publishing; 2002. 5. Kirmayer LJ. Culture and anxiety: a clinical and research agenda. Cultural issues in the treatment of anxiety New York: Guilford; 1997. 6. Asnaani A, Gutner CA, Hinton DE, Hofmann SG. Panic Disorder, Panic Attacks and Panic Attack Symptoms across Race‐ Ethnic Groups: Results of the Collaborative Psychiatric Epidemiology Studies. CNS Neurosci Ther. 2009;15(3):249-54. 7. Cho MJ, Kim J-K, Jeon HJ, Suh T, Chung I-W, Hong JP, et al. Lifetime and 12-month prevalence of DSM-IV psychiatric disorders among Korean adults. J Nerv Ment Dis. 2007;195(3):203-10. 8. Varela RE, Hensley-Maloney L. The influence of culture on anxiety in Latino youth: A review. Clin Child Fam Psychol Rev. 2009;12(3):217-33. 9. Selim N. Cultural dimensions of depression in Bangladesh: a qualitative study in two villages of Matlab. J Health Popul Nutr. 2010;28(1):95-106. 10. Lewis‐ Fernández R, Hinton DE, Laria AJ, Patterson EH, Hofmann SG, Craske MG, et al. Culture and the anxiety disorders: recommendations for DSM‐ V. Depress Anxiety.
- 88. 2010;27(2):212-29. 11. Hofmann SG, Asnaani A, Hinton DE. Cultural aspects in social anxiety and social anxiety disorder. Depress Anxiety 2010; 27: 1117-1127. 12. Regier DA, Kuhl EA, Kupfer DJ. The DSM‐ 5: Classification and criteria changes. World Psychiatry. 2013;12(2):92-8. 13. Zarean M, Shahidi S, van de Vijver FJ, Dehghani M, Asadollahpour A, Sohrabi R. Reflections from Indigenous Psychology on Emotional Disorders: A Qualitative Study from Iran. International Journal of Applied Behavioral Sciences 2014;1(2):19-26. 14. Hoge EA, Tamrakar SM, Christian KM, Mahara N, Nepal MK, Pollack MH, et al. Cross-cultural differences in somatic presentation in patients with generalized anxiety disorder. J Nerv Ment Dis. 2006;194(12):962-6. 15. Lee S, Tsang A, Chui H, Kwok K, Cheung E. A community epidemiological survey of generalized anxiety disorder in Hong Kong. Community Ment Health J. 2007;43(4):305-19. Cultural Aspects of Social Anxiety Disorder Iranian J Psychiatry 14: 1, January 2019 ijps.tums.ac.ir 39 16. Richerson PJ. Cultural Evolution and Gene–
- 89. Culture Coevolution. Evolutionary Studies in Imaginative Culture 2018;1(1):89-92. 17. Dressler WW, Balieiro MC, de Araújo LF, Silva WA, dos Santos JE. Culture as a mediator of gene-environment interaction: Cultural consonance, childhood adversity, a 2A serotonin receptor polymorphism, and depression in urban Brazil. Soc Sci Med. 2016;161:109-17. 18. Green J, Thorogood N. Qualitative methods for health research: Sage; 2018. 19. Hayes N. Doing psychological research: Taylor & Francis Group Abingdon; 2000. 20. Association AP. Diagnostic and statistical manual of mental disorders (DSM-5®): American Psychiatric Pub; 2013. 21. Dinnel DL, Kleinknecht RA, Tanaka-Matsumi J. A cross-cultural comparison of social phobia symptoms. Journal of Psychopathology and Behavioral Assessment 2002; 24(2): 75-84. 22. Dejman M. Cultural explanatory model of depression among Iranian women in three ethnic groups (Fars, Kurds and Turks): Institutionen för klinisk neurovetenskap/Department of Clinical Neuroscience; 2010. 23. Kirmayer LJ, Young A. Culture and somatization: clinical, epidemiological, and ethnographic perspectives. Psychosom Med.
- 90. 1998;60(4):420-30. 24. Beck JS. Cognitive behavior therapy: Basics and beyond: Guilford press; 2011. 25. Andrew G, Cohen A, Salgaonkar S, Patel V. The explanatory models of depression and anxiety in primary care: a qualitative study from India. BMC Res Notes. 2012;5:499. 26. Barrera TL, Norton PJ. Quality of life impairment in generalized anxiety disorder, social phobia, and panic disorder. J Anxiety Disord. 2009;23(8):1086-90. 27. Rasic D, Robinson JA, Bolton J, Bienvenu OJ, Sareen J. Longitudinal relationships of religious worship attendance and spirituality with major depression, anxiety disorders, and suicidal ideation and attempts: Findings from the Baltimore epidemiologic catchment area study. J Psychiatr Res. 2011;45(6):848-54. Copyright of Iranian Journal of Psychiatry is the property of Tehran University of Medical Sciences and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print,
- 91. download, or email articles for individual use. ©2013, ALL RIGHTS RESERVED ISSN: 1555–7855 16 INTERNATIONAL JOURNAL OF BEHAVIORAL CONSULTATION AND THERAPY 2013, VOL. 7, NO. 4 Social Anxiety Disorder and Social Skills: A Critical Review of the Literature Antonio Paulo Angélico1, José Alexandre S. Crippa2 and Sonia Regina Loureiro2 1São João del-Rei Federal University and 2São Paulo University Abstract The objective of this article is to present a critical analysis of the research outlines used in empirical studies published between the years 2000 and March of 2007 about social anxiety disorder and its associations with social skills. Seventeen papers were identified and grouped into two classes for analysis, namely: Characterization of Social Skills Repertoire (N = 10) and Therapeutical Modalities – Application and Comparison of Clinical Intervention (N = 7). The critical analysis of the research outlines pointed to the necessity of new studies with clinical and non-clinical samples, with random allocation of individuals, with the proposition of contextualized