Assessing the efficacy of targeted therapy using circulating epithelial tumor...
The Convergence of Endothelin and Androgen Signaling in the Metastasis of Prostate Cancer
1. The
Convergence
of
Endothelin
and
Androgen
Signaling
in
the
Metastasis
of
Prostate
Cancer
to
Bone
Alexander
Smith1,
Katrina
Clines2,
Diondra
Harris2,
Hyun
SikMoon2 Gregory
Clines2,3
1University
of
Michigan
Undergraduate
Research
Opportunity
Program;
2University
of
Michigan
Department
of
Internal
Medicine;
3Veteran
Affairs
Hospital,
Ann
Arbor,
MI
Introduction
Endothelin-‐1
(ET-‐1)
has
a
variety
of
biological
actions.
In
respect
to
its
role
in
cancer
biology,
endothelin-‐1
is
secreted
by
prostate
cancer
cells
metastatic
to
bone
and
activates
the
endothelin
A
receptor
(ETAR)
on
osteoblasts
to
increase
differentiation
and
proliferation
that
ultimately
produces
an
osteosclerotic
response.
It
is
thought
that
this
then
changes
the
bone
microenvironment
to
make
metastatic
prostate
cancer
cells
more
hospitable
for
residency
and
growth.
Initial
clinical
trials
testing
the
ETAR
antagonist
zibotentan in
combination
with
the
standard
androgen
deprivation
therapy
at
that
time
showed
no
benefit.
Preliminary
data
from
our
laboratory
suggests
that
newer
medications
(abiraterone and
enzalutamide)
now
approved
in
men
with
metastatic
prostate
cancer
that
more
effectively
reduce
androgens
may
in
fact
increase
the
effectiveness
of
zibotentan.
Hypothesis
ETAR
blockade
reduces
prostate
cancer
progression
and
bone
metastasis
when
combined
with
modern
and
complete
androgen
deprivation
therapy.
Abstract
Prostate
cancer
is
the
most
common
non-‐skin
cancer
in
men.
This
malignancy
is
responsible
for
more
than
27,000
deaths
in
the
United
States
in
2015.
Androgens
are
critical
for
prostate
cancer
cell
survival.
Androgen
deprivation
therapy
is
often
prescribed
in
the
initial
treatment
of
early
prostate
cancer.
While
initially
successful,
this
therapy
often
becomes
ineffective
as
the
cancer
progresses
and
transforms
to
androgen
independence.
While
the
survival
rate
for
prostate
cancer
in
the
early
stages
is
nearly
100%,
the
survival
rate
drops
to
a
dismal
29%
when
prostate
cancer
has
metastasized
to
bone.
Endothelin-‐1
(ET-‐1)
is
a
peptide
hormone
with
a
variety
of
biological
functions,
including
an
importance
in
cancer
biology.
ET-‐1
is
secreted
by
prostate
cancer
cells
metastatic
to
bone
where
it
activates
the
endothelinA
receptor
(ETAR)
on
osteoblasts,
leading
to
the
formation
of
characteristic
osteosclerotic
lesions.
There
is
evidence
that
endothelinsignaling
converges
with
androgen
signaling
such
that
the
combined
blockade
may
in
fact
may
have
greater
benefit
than
each
treatment
alone.
Preliminary
animal
experiments
involving
combined
ETAR
blockade
and
androgen
deprivation
revealed
a
significant
survival
advantage
and
a
decrease
in
tumor
events
compared
to
each
of
these
interventions
alone.
The
aims
of
this
project
are
to
understand
the
mechanisms
by
which
ET-‐1
and
androgen
signaling
converge
in
prostate
cancer,
in
order
to
develop
improved
therapies
for
metastatic
disease.
The
in
vitro component
of
this
larger
experiment
has
paralleled
the
results
we
have
seen
in
animal
models
thus
far.
The
goals
of
this
study
are
to
assess
changes
in
proliferation,
apoptosis,
in
vitro invasion
and
epithelial-‐to-‐
mesenchymal transition
(EMT)
with
androgen
treatment,
ETAR
blockade
and
the
combined
interventions
in
prostate
cancer
cells.
Although
we
did
not
detect
changes
in
proliferation
with
ETAR
blockade,
an
interaction
with
the
EMT
marker
E-‐cadherin
was
detected
with
ETAR
blockade
and
androgen
treatment.
Aims
Aim
1:
Determine
the effects
of
combined
ETAR
blockade
and
androgen
deprivation
in
an
animal
model
of
bone
metastasis
and
in
human
prostate
cancer
cells
If
ETAR
blockade
reduces
prostate
cancer
progression
and
bone
metastasis
when
combined
with
modern,
effective
ADT,
we
expect
to
see
differences
in
characteristics
1. In
vivo
prostate
cancer
metastasis
to
bone
2. In
vitro
cellular
changes
(epithelial
to
mesenchymal
transition
markers
(EMT),
apoptosis,
and
invasion)
Aim
2:
Determine
the
effects
of
ET-‐1
in
transmitting
cellular
androgen
signals
in
prostate
cancer
cells
We
will
be
assessing
the
effects
of
ET-‐1
on
the
following
characteristics.
This
combination
of
tests
will
reveal
the
effects
ET-‐1
has
on
androgen
at
a
mechanistic
level.
1. Androgen
receptor
Responsive
Genes
2. Androgen
Secretion
3. Androgen
receptor
Expression
Methods
In
Vivo
Studies
Male
athymic
nude
mice
underwent
castration
or
sham
surgery
at
4
weeks
of
age.
At
5
weeks
of
age,
animals
underwent
intracardiac
inoculation
of
the
human
prostate
cancer
cell
line
ARCaPM.
After
recovery,
mice
were
administered
zibotentan
10
mg/kg/day
for
5
days/week
or
vehicle
control
by
gavage.
The
four
treatment
groups
mentioned
above,
with
each
consisting
of
twelve
mice,
were
studied.
Mice
were
monitored
daily
for
complications
and
periodically
by
X-‐ray
to
detect
bone
lesions.
The
vehicle
+
sham,
vehicle
+
castration,
and
zibotentan
+
sham
groups
exhibited
reduced
survival
and
exhibited
tumors
either
by
X-‐ray
or
by
visual
inspection
and
euthenasia.
All
animals
in
the
zibotentan
castration
group
survived
until
the
completion
of
the
experiment
and
exhibited
no
X-‐ray
or
visual
evidence
of
tumor.
In
Vitro
Studies
ARCaPM and
C4-‐2B
cell
lines
were
plated
at
75%
confluency
and
were
allowed
to
replicate
for
one
hour
before
being
administered
zibotentan (10
μM)
or
control.
One
hour
after
administering
zibotentan,
the
cells
were
treated
with
DHT
(10
nM)
or
control.
Each
combination
resulted
in
the
four
treatment
groups
above
.
The
cells
were
then
incubated
at
37
degrees
Celsius
for
48
hours.
To
assess
EMT
markers,
RNA
was
prepared
at
the
end
of
the
two
day
period
using
a
standard
protocol. The
following
epithelial
to
mesenchymal
transition
markers
will
be
measured:
TWIST,
SLUG,
SNAIL,
E-‐
CADHERIN,
and
N-‐CADHERIN. The
quantification
of
these
EMT
markers
using
RTqPCR
will
be
measured
against
RPL32 – an
EMT
marker
that
is
relatively
constant
in
its
expression
across
treatment
groups.
Equivalent
Treatment
Groups
In vitro
studies In
vivo
studies
1 -‐Zibo
+Dihydrotestosterone(DHT)
Vehicle
+
Sham
2 -‐Zibo
-‐DHT Vehicle
+
Castration
3 +Zibo +DHT Zibo +
Sham
4 +Zibo
-‐DHT
Zibo
+
Castration
Results
After
intracardiac
inoculation,
characteristic
osteolytic
lesions
were
detected
by
X-‐
ray
starting
at
about
4
weeks
post-‐inoculation
(Figure
1).
These
lesions
grew
in
size
over
time.
Survival
was
monitored
in
the
four
treatment
groups
(Veh+Sham,
Veh+Castr,
Zibo+Sham,
Zibo+Castr).
All
animals
in
the
Zibo+Castr group
survived
until
the
end
of
the
experiment
without
evidence
of
tumor
(Figure
2).
In
fact,
the
Zibo+Sham groups
exhibited
the
lowest
survival.
We
also
categorized
the
groups
by
time
to
the
development
of
any
radiographic,
clinical
and
visual
signs
of
tumor.
Again,
the
Zibo+Castr group
revealed
no
evidence
of
tumor.
The
other
three
groups
developed
tumor
at
the
same
rate.
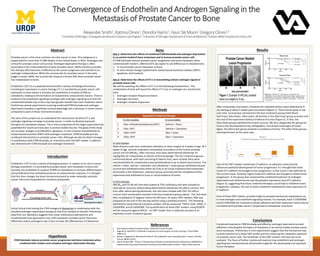
One
of
the
EMT
markers
tested
was
E-‐Cadherin:
an
adhesion
molecule
that
influences
epithelial
development
of
tumor
progression.
It
is
thought
that
lower
levels
of
E-‐cadherin
encourages
tumor
progression,
as
the
tumor
is
less
adhered
to
the
current
tissue.
Similarly,
higher
levels
of
E-‐cadherin
are
thought
to
inhibit
tumor
progression.
In
the
group
that
contained
the
combined
treatment
of
androgen
deprivation
and
zibotentan
we
saw
the
greatest
expression
level
of
E-‐cadherin
(Figure
3),
suggesting
that
these
combined
therapies
could
lead
to
inhibited
tumor
progression.
Likewise,
the
lack
of
either
treatment
exhibited
the
least
expression
of
E-‐Cadherin.
Each
of
these
EMT
markers
provide
insight
to
possible
mechanistic
explanations
as
to
how
androgen
and
endothelin
signaling
interact.
For
example,
both
E-‐CADHERIN
and
N-‐CADHERIN are
involved
in
cellular
adhesion
and
their
expression
levels
may
be
correlated
with
prostate
cancer’s
propensity
to
metastasize
onto
bone.
Conclusions
Combined
treatments
ETAR
blockade
and
effective
androgen
deprivation
proved
effective
in
blocking
the
formation
of
metastasis
in
an
animal
model
prostate
cancer
bone
metastasis.
Preliminary
in
vitro
experiments
suggest
that
the
mechanism
may
include
induction
of
a
lower
EMT
profile
and
thus
reducing
the
metastatic
potential
of
prostate
cancer
cells. The
remainder
of
the
EMT
markers
still
have
yet
to
be
analyzed.
The
focus
of
further
studies
will
examine
how
endothelin
and
androgen
signaling
are
intertwined
and
will
provide
insight
for
the
development
of
improved
future
therapies.
References
1. Key
Statistics
about
Prostate
Cancer.
American
Cancer
Society
2. Bagnato A,
Natali
PG.
Endothelin
receptors
as
novel
targets
in
tumor
therapy.
J
Transl Med
2004:2:16
3. Nelson
J,
Bagnato A,
BattistiniB,
Nisen P.
The
endothelin
axis:
emerging
role
in
cancer. Nat
Rev
Cancer
2003;3:110-‐6
4. Joel
B.
Nelson
MD,
“Phase
3,
Randomized,
Placebo-‐Controlled
Study
of
Zibotentan (ZD4054)
in
Patients
with
Castration-‐Resistant
Prostate
Cancer
Metastatic
to
Bone.”
Wiley
Online
Journal
1 1.92
6.49
14.6
0
5
10
15
20
-‐Zibo,
'-‐DHT -‐Zibo,
'-‐DHT +Zibo,
'+DHT +Zibo,
'-‐DHT
Expression
Levels
Relative
to
RPL32
Treatment
groups
Figure
3
E-‐Cadherin
Expression
in
C42B
Prostate
Cancer
Cells