
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Oral submucous fibrosis
Similar to Oral submucous fibrosis (20)
More from Ajins Thudhupillyl
Recently uploaded
Recently uploaded (20)
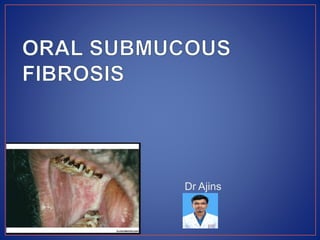
Oral submucous fibrosis
- 1. Dr Ajins
- 2. INTRODUCTION: Oral precancerous condition is a generalized pathological state associated with a significantly increased risk of cancer according to World Health Organization (WHO) in 1978. Oral submucous fibrosis is a premalignant condition affecting any part of oral cavity & sometimes the pharynx. Oral submucous fibrosis is a chronic progressive scarring disease that predominantly affects the people of South East Asian origin. This condition was described by Schwartz in 1952 designated the condition as “oral Submucous fibrosis”.
- 3. SYNONYMS: • Atrophia Idiopathica • Tropica mucosae orali • Idiopathic scleroderma of the mouth • Idiopathic palatal fibrosis • Sclerosing stomatitis • Juxta-Epithelial fibrosis (Juxta means near)
- 4. DEFINITION Oral submucous fibrosis is a slowly progressive chronic fibrotic disease of the oral cavity and oropharynx; characterized by fibro elastic change and inflammation mucosa, leading to a progressive inability to open the mouth, swallow or speak. ETIOLOGY PRIMARY FACTORS: Habitual use of betel and its constituents, which include areca nut (areca catechu), leaf to betel pepper (piper betel), and lime (CaOH2). OTHER FACTORS : Nutritional & Vitamin deficiencies. Hypersensitivity of chili pepper, chewing tobacco etc. Tobacco, Lime & Betel Quid Chronic Candidiasis (In fungal infection → Yeasts → produce carcinogen mainly nitrosamine → malignant transformation.) Genetic Abnormalities HSV/HPV Autoimmunity( In HLA-DR3 antigen (+) ce of serum immunoglobulins and autoantibodies )
- 5. PATHOGENESIS OF OSMF Areca products contain high level of copper (mean 302 nml/g)(Daily intake → 0.6-1.6 mg) Copper intake → Increased Lysyl oxidase activity →Increase in collagen cross- linkage- Fibrotic disorder like OSMF, Hepatic &pulmonary fibrosis, Scleroderma. Areca nut chewing → Copper > 5mg/ day. Arecoline, an active alkaloid found in betel nuts, simulates fibroblasts to increase production of collagen. Arecanut decreases the secretion of collagenase. Deficiency in collagen phagocytosis by OSF fibroblasts. Stabilization of collagen structure by catechin and tannins from the arecanut. Ingestion of chilies ( capsaicin, active ingredient of chilies, stimulates widespread palatal fibrosis in rats)
- 6. CLINICAL FEATURES: The onset is insidious over 2-5 years period Prodromal symptoms include; Burning sensation in the mouth when consuming spicy food Appearance of blister especially in the palate; ulceration or generalized inflammation of the oral mucosa Excessive salivation; defective gustatory sensation & dryness of the mouth Early stage → Focal vascular dilatations clinically manifests as petechiae (may be vascular response due to hypersensitivity of oral mucosa to some irritants like chilly) Petechiae were observed mostly in the tongue followed by labial and buccal mucosa with no sign of blood dyscrasia or systemic disorders There is pain on palpation on the areas where the submucosal fibrotic bands are developing.
- 7. Advanced OSMF: As the disease progresses, oral mucosa become blanched and slightly opaque and white thick fibrous band appear Oral mucosa is symmetrically involved & fibrous band in the oral mucosa run in vertical direction. It is preceded by and/or associated with vesicle formation and is always associated with juxta epithelial inflammatory reaction followed by progressive hyalinization of lamina propria. Later → Sub epithelial and sub mucosal myofibrosis leads to stiffness of oral mucosa and deeper connective tissue with progressive limitation in opening of the mouth and protrusion of tongue leading to difficult in eating, swallowing and phonation.
- 8. Severe cases →Deviation of uvula Inability to whistle or blow a candle. Pterygomandibular raphe involvement → Limitation of mouth opening Most of the patient experience a protracted period of stomatitis and/or glossitis with remission and exacerbation. If fibrosis involves pharynx→ patient experience referred pain in ear. Nasal voice as one of the later signs in some patients.
- 13. • Atrophic oral epithelim that may show atypia and dysplasia • Diffuse hyalinization of the subepithelial stroma with pigment incontinence from the ovelying epithelial melanin • Intercellular edema with or withot hyperkeratosis,parakeratosis or orthokeratosis. • EARLY STAGE: • Epithelial hyperplasia,marked oedema,thickened collagen bundles,moderate numbers of large fibroblasts,dilated and congested blood vessels and inflammatory cell infiltration containing a number of polymorphonuclear leukocytes.
- 14. • ADVANCED STAGE: • Epithelial atropy • Dense bundles and sheets of collagen • Thick bands of subepithelial hyalinization extending into the submucosal tissues • Decreased vascularity • No oedema • Decreased inflamatory cells are found
- 15. • Buccal mucosa • Facial pillars • Soft palate • Lips and • Hard palate • The fibrous bands in the buccal mucosa run in the vertical direction , sometimes so marked that the cheeks are almost immovable.
- 16. • Decreased hemoglobin level • Decreased iron level • Decreased protein level • Increased erythrocyte sedimentation rate • Decreased vitamin B levels.
- 17. MANAGEMENT: • Reduction or even elimination of the habit of arecanut chewing. • Nutritional support: Mainly for high proteins and calories and for vitamin B complex and other vitamins and minerals. Vitamin A supplements are excellent sources of anti-oxidants. • Immunomodulatory drugs: Local and systemic application of glucocorticoids and placental extracts. • Physiotherapy: Forceful mouth opening and heat therapy. • Ask the patient to stand in front of the mirror and cause mouth opening by holding hands over the two arches and stretching. • Ask the patient to blow the balloon atleast three times a day. • Patient can place bundles of ice-cream stick in the posterior part of the mouth and ask them to increase the sticks day by day.
- 18. • Local drug delivery: Local injection of corticosteroids, Placental extracts and hyaluronidase. Oral iron preparations. • Combined therapy: With peripheral vasodilators, vitamins D, E, A and B complex, iodine, placental extract, local and systemic corticosteroids and physiotherapy claim a high success rate in management of OSMF. • Surgical management: Submucosal resection of the fibrotic bands and replacement with a partial thickness skin or mucosal graft. Bilateral temporalis myotomy. Surgery seems to be a poor option in the treatment of oral submucous fibrosis since the more fibrosis and disability on resecting the bands. PROGNOSIS : It is a premalignant condition. Malignant transformation rate is 4 – 13%
- 19. • THANKYOU !