
Recommended
More Related Content
Similar to Facial Nerve.pptx
Similar to Facial Nerve.pptx (20)
More from Adhishesh Kaul
Recently uploaded
Recently uploaded (20)
Facial Nerve.pptx
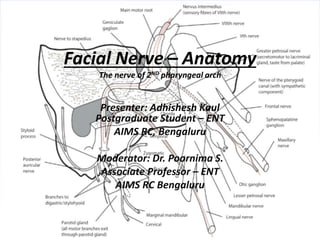
- 1. Facial Nerve – Anatomy The nerve of 2ND pharyngeal arch Presenter: Adhishesh Kaul Postgraduate Student – ENT AIMS RC, Bengaluru Moderator: Dr. Poornima S. Associate Professor – ENT AIMS RC Bengaluru
- 3. “Cranial nerves are the conduits by which the brain receives information directly from, and controls the functions of, structures that are mainly but not exclusively in head and neck”
- 4. Arch Nerve Muscle Skeletal Structure Ligament 2nd Arch (Hyoid Arch) Facial Nerve (VII nerve) Muscle of facial expression Stapes Stylohyoid ligament Stapedius Styloid process Stylohyoid Lesser cornu of hyoid Posterior belly of digastric Upper part of body of Hyoid Structures from 2nd Brachial Arch
- 6. Functional Components SENSORY COMPONENT • General Visceral Afferent • Special Visceral Afferent • General Somatic Afferent MOTOR COMPONENT • Special Visceral Efferent • General Visceral Efferent
- 7. We have a Neural tube and Sulcus limitans Sulcus limitans divides NT into 1. Alar Plate (Dorsal Part – represents dorsal horn of spinal cord and is SENSORY in function) 2. Basal Plate (Ventral Part – represents ventral horn of spinal cord and is MOTOR in function)
- 9. • CN nuclei developing in – ALAR PLATE – SENSORY – BASAL PLATE – MOTOR
- 10. • Neural Tube opens to accommodate – 4th Ventricle • Sensory Nuclei (afferent) – develop in Alar plate • Motor Nuclei (efferent) – develop in Basal Plate
- 11. What is this SVE, GVE, GVA, etc? • The neurons form cell columns, which are divided by anatomists into functional categories. • Cell columns are divided into – Motor vs Sensory – General vs Special – Somatic vs Visceral
- 13. Motor Nuclei • nerves from General Somatic Efferent – supply skeletal muscles • nerves from General Visceral Efferent – supply smooth muscles • nerves from Special Visceral Efferent – supply muscles from pharyngeal arches
- 14. Sensory Nuclei • nerves from General Visceral Afferent: for general sensation from viscera – temperature, touch, pressure • nerves from Special Visceral Afferent: for special sensation from the viscera – taste • nerves from General Somatic Afferent: for general sensations from the skeletal muscles
- 15. So what all cell columns is facial nerve involved with?
- 16. Functional Components SENSORY COMPONENT • General Visceral Afferent • Special Visceral Afferent • General Somatic Afferent MOTOR COMPONENT • Special Visceral Efferent • General Visceral Efferent
- 18. Cranial Nerve Nuclei “Cranial nerves which attach to brain stem are associated with a number of cell groupings of varying size referred to as cranial nerve nuclei”
- 19. Facial Nerve Nuclei Fibres of facial nerve are connected to 4 nuclei in lower Pons • Motor Nucleus – deep reticular formation of lower pons • Parasympathetic Nuclei – posterolateral to motor nucleus – Superior Salivatory nucleus: afferent from hypothalamus and NTS – Lacrimal Nucleus: from hypothalamus for emotional, sensory nuclei of CN V for reflex lacrimation • Sensory Nucleus – is upper part of Nucleus of tractus solitarius.
- 22. Motor Nucleus • Site: deep in reticular formation of pons anterior and cranial to nervus intermedius lateral surface of brain stem, close to lower border of pons • Supply: Upper part of face: receives corticonuclear fibres from both motor cortex Lower part of face: receives corticonuclear fibres only from opposite cortex
- 27. Intracranial Intratemporal Extracranial/ Extratemporal Course 25mm in length (atlas of facial nerve) 15mm (dhingra) ~33mm in length XX mm in length Segments 1. Meatal 2. Labyrinthine 3. Horizontal/ Tympanic 4. Vertical/ Mastoid FACIAL CANAL
- 29. Course INTRACRANIAL EXTRACRANIAL ENTERS TEMPORAL BONE THROUGH IAM IN PETROUS PART OF TEMPORAL BONE (IN TEMPORAL BONE) LEAVE: IAM ENTERS: FACIAL CANAL AFTER LEAVING CRANIUM AND FACIAL CANAL THROUGH SMF EVENTS IN FACIAL CANAL: (Z-SHAPE STR) 1. 2 ROOTS FUSE IN MEATUS 2. NERVE FORMS GENICULATE GANGLION 3. NERVE GIVES RISE TO ITS 3 BRANCHES
- 31. Course of Facial Nerve • Roots (at brain stem): – Motor: • supply muscles of face – Sensory (nervus intermedius): • perception of taste • Parasympathetic fibres to lacrimal glands/ submandibular gland/ sublingual gland • Attached to lower part of Pons – medial to CN VIII
- 33. • Emerges from brainstem at junction of Pons and Medulla (pontomedullary junction – 1.5mm anterior to CN VIII) • Till Internal Acoustic Meatus: Lateral + Forward (rostolateral course) (with CN VIII) through cerebellopontine cistern across posterior cranial fossa in subarachnoid space TO ENTER INTERNAL AUDITORY CANAL
- 35. • Emerges from brainstem at junction of Pons and Medulla (pontomedullary junction – 1.5mm anterior to CN VIII) • Till Internal Acoustic Meatus: Lateral + Forward (rostolateral course) (with CN VIII) through cerebellopontine cistern across posterior cranial fossa in subarachnoid space TO ENTER INTERNAL AUDITORY CANAL
- 36. • Relation to artery: – Anterior Inferior Cerebellar Artery, may lie Anterior or posterior or loop around or pass between the nerves • IN CP ANGLE SURGERIES, THIS ARTERY MUST BE PRESERVED • AICA supplies: Labyrinthine artery
- 38. CP angle cistern CP angle cistern is triangular CSF filled cistern between anterior surface of cerebellum and lateral surface of pons Related structures – AICA – CN VII, CN CN VIII – Foramen luschka
- 39. Intratemporal Course • Segments – Meatal – Labyrinthine – from meatal foramen to geni. gang. – Tympanic – Mastoid
- 41. Course in IAC/ Meatal Segment (IAC: location: anterior to superior SCC) In IAC location of CN VII: Ant Sup Quad Enters Fallopian canal/Facial Canal at fundus of IAC (at entrance of fallopian canal (meatal foramen), FN is narrowest 0.61mm)
- 43. Meatal Segment • FN enters Temporal bone through IAM on posteromedial surface of petrous ridge • Motor and sensory roots join at fundus/ base of IAM • It is located on the ant sup quad of IAM above falciform crest, anterior to bill bar These are important landmark for facial nerve via translabyrinthine, transcochlear and middle cranial fossa approach Bill Bar: divides superior quad of IAM into Ant and Post quad (named after William Fouts House)
- 44. Course within Facial Canal Facial Canal: runs across medial wall and down posterior wall of tympanic cavity to Stylomastoid foramen 3 Parts of Facial Nerve in Facial Canal Course: Lateral and Forward • 1st Part: directed laterally above vestibule • 2nd Part: runs backward in relation to medial wall of middle ear • 3rd Part: directed vertically downward – behind the promontory
- 46. • Enters Fallopian canal/Facial Canal at fundus of IAC • As the FN enters FC, FC has a bend that contains geniculate ganglion • Branches in temporal bone –(explained ahead) can be divided into – From geniculate ganglion – Arise within facial canal
- 47. Labyrinthine Segment • From fallopian canal/ facial canal • Course: – Anterior-lateral course between and superior to cochlea and vestibule – Turns back on geniculate ganglion (Geniculate ganglion resides in distal part of labyrinthine segment) • Relation: Covered by superior part of petrous bone Runs over junction of cochlea and vestibule
- 48. Tympanic Segment • ~11mm long • From: Geniculate ganglion (genu) • Runs between lateral semicircular canal superiorly and the stapes inferiorly • Forms the superior margin of the fossa ovale • Relation: Below FN – Promontory (basal turn of cochlea) and Oval window (fenestra vestibuli) Above FN – Ampullary end of SCC
- 50. Mastoid Segment • ~13mm long • From: Posterior end of Fenestra Vestibuli • Course in Bony posterior wall of middle ear • Direction: Downward and lateral • Nerve exits at anterior margin of digastric groove, behind root of styloid • Relation: Posterior FN: Mastoid Antrum
- 51. Extracranial Course • Exit: Stylomastoid foramen at 2.5cm – 4cm deep to middle of anterior border of mastoid (9mm from post belly of digastric and 11mm from bony EAC) • Course: – Crosses lateral side of base of styloid process – Enters: Parotid at Posteromedial surface – Runs forward and downward behind mandibular ramus – Crosses retromandibular vein and ECA – Behind neck of mandible divides into 5 terminal branches
- 53. Relation with Parotid Gland • FN divides the gland into Suprafacial and Subfacial parts • Tracing – Forward : expose trunk at SMF: 1cm FN before entry into parotid: 1cm after it enters but before it divides Temporofacial and Cervicofacial: use to make plane of cleavage – Traced backward from terminal branches
- 55. Branches of Facial Nerve • Within Facial Canal Greater petrosal nerve (from geniculate ganglion) Nerve to stapedius (behind pyramidal eminence of post wall of tympanic cavity) – at level of 2nd genu Chorda tympani • At Exit from Stylomastoid Foramen Posterior Auricular (supply occipetal belly of occipetofrontalis) Digastric Stylohyoid • Terminal Branches • Communicating branches with adjacent CN
- 56. Terminal Branches • Temporal • Zygomatic • Buccal • Mandibular (marginal mandibular) • Cervical
- 58. Greater Petrosal Nerve • Fibres for Pterygopalatine ganglion and taste fibre from palate • Branch of: Nervus Intermedius • Receives a branch from: Tympanic Plexus • Course: – Passes anteriorly – Transverses hiatus on ant surface of petrous part of temporal bone – Enters middle cranial fossa and runs forward on the groove above lesser petrosal nerve – Passes beneath trigeminal ganglion to reach foramen lacerum – Joined by deep petrosal nerve to become VIDIAN NERVE
- 59. Chorda Tympani • Leaves FN 6mm above SMF • Arises from middle of vertical segment • Secretomotor fibre to submandibular and sublingual gland • Runs: anterosuperiorly in canal enter tympanic cavity via posterior canaliculus curves anteriorly in substance of Tym Membrane crosses medial to upper part of handle of malleus to ant wall enters ant. Canaliculus exits skull/tympanic cavity at petrotympanic fissure
- 62. Posterior Auricular Nerve • Supplies: pinna, occipital belly of occipitofrontalis • Communicates with auricular branch of vagus
- 63. Distribution of Facial Nerve Branches
- 65. Blood Supply of Facial Nerve • Anterior Inferior Cerebellar artery: supply CP angle • Labyrinthine artery: br of A-I cerebellar art., supply IAC • Superficial Petrosal artery: br of MMA, supply Geni. gangli. • Stylomastoid artery: br of post. auricular art., supply mastoid and tympanic
- 67. Variation and Anomaly of Facial Nerve • Bony dehiscence: mc in tympanic segment over oval window> region near geniculate ganglion> retrofacial mastoid • Prolapse of nerve: dehiscent nerve may prolapse over stapes and make stapes surgery/ ossicular reconstruct difficult • Hump: posteriorly: vulnerable while exposing antrum • Bifurcation and trifurcation: vertical part divides • Bifurcation and enclosing the stapes: division proximal to oval window with one part above and one part below, then rejoining • Between oval and round window: before oval window nerve crosses middle ear passing between oval and round window
- 69. In cholesteatoma, facial nerve may 1. Lie under the bone 2. Be dehiscent (congenitally or acquired due to cholesteatoma) 3. Be protuberant Hence great caution must be exercised in removing cholesteatoma from extensively eroded facial nerve, esp when protuberant or inflame
- 71. Lesions of Facial Nerve Upper Motor Neuron • Lesion above the FN nucleus in Pons • Paralysis: Lower half of the face as upper part is supplied by both the hemispheres. Lower Motor Neuron • Lesion at FN nucleus in Pons or distal to it. • Site: by topodiagnostic test – Homolateral lacrimation – Stapedial reflex – Homolateral submandibular salivation – Taste from homolateral anterior 2/3 tongue
- 72. UMN vs LMN Lesion
- 74. • Schimers Test: proximal to greater petrosal nerve (geniculate ganglion) • Stapedial relex: proximal to nerve to stapedius (tympanic segment) • Salivary flow test: proximal to chorda tympani nerve (mastoid/ vertical segment) • Taste Test: proximal to chorda tympani nerve (mastoid/ vertical segment)
- 76. Other Clinical Aspects • Before mastoid development in child, FN lies subcutaneously and is at a danger of being cut if any postauricular incision is given too deep. • 1st brachial arch anomalies are associated with facial nerve, that they’re either superficial to it or deep • Radical neck dissection, mandibular branch of facial nerve is to be identified and preserved.
- 77. Centrally localized lesions • Preganglionic secretion fibers to the lacrimal gland: These branch off from the nerve at the geniculate ganglion into the greater superficial petrosal nerve. A lesion in the preganglionic or ganglionic segments leads to unilateral impairment of lacrimal secretion. A Schirmer test for pathologic values can be useful for detection. • Preganglionic secretion fibers to the submandibular gland: These exit the nerve together with the chorda tympani. Damage in the tympanic portion causes reduced ipsilateral saliva production of the submandibular gland. A sialometry test is used (cannulation and collection of whole saliva). A pathologic sialogram, along with remarkable Schirmer values on the same side, are a sign of damage in the tympanic portion of the nerve course. If the Schirmer test is additionally positive, the lesion can be presumed to be more centrally localized (usually in the labyrinthine portion). • Motor fibers to the stapedius muscle: Damage occurring proximal to the pyramidal process causes reflex dysfunction or increased reflex threshold on the injured side.
- 78. References 1. Anatomy for plastic surgery of the face, head and neck 2. B D Chaurasia’s Human Anatomy, ed 8 3. Clinical Neuroanatomy, Richard S. Snell, ed 7 4. Cummings Otolaryngology Head and Neck Surgery, ed 6 5. Disease of ear, nose and throat and head and neck surgery, ed 6 6. Entokey 7. Gray’s Anatomy for Students, ed 3 8. Gray’s Clinical Neuroanatomy 9. Lee McGregor’s Synopsis of Surgical Anatomy, ed 12 10. Scott-Brown’s Otorhinolaryngology Head & Neck Surgery, ed 8 11. Snell’s Clinical Anatomy
Editor's Notes
- Temporal: frontalis, orbicularis, corrugator Zygomatic: orbicularis Buccal: orbicularis, zygomaticus Marginal mandibular: mentalis, depressor labii, Cervical: Platysma
- Brain stem: Medulla, pons, midbrain