Al Razi Acute Pain Service Audit 2012 2013
•
1 like•521 views

This document summarizes pain service audits conducted in 2012 and 2013 at a hospital. The 2012 audit found issues like incomplete pain assessment documentation, high pain scores without timely intervention, and high catheter dislodgement rates. Solutions proposed included encouraging complete documentation, following up on high pain scores sooner, and improving catheter fixation. The 2013 audit found improvements in some areas like documentation but also an increase in missing patient records. Continuing to emphasize proper documentation follow up was recommended.

Recommended
Recommended
More Related Content
What's hot
What's hot (18)
Similar to Al Razi Acute Pain Service Audit 2012 2013
Similar to Al Razi Acute Pain Service Audit 2012 2013 (20)
More from Farah Jafri
More from Farah Jafri (7)
Recently uploaded
Recently uploaded (20)
Al Razi Acute Pain Service Audit 2012 2013
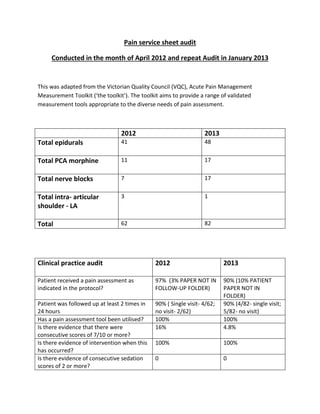
- 1. Pain service sheet audit Conducted in the month of April 2012 and repeat Audit in January 2013 This was adapted from the Victorian Quality Council (VQC), Acute Pain Management Measurement Toolkit (‘the toolkit’). The toolkit aims to provide a range of validated measurement tools appropriate to the diverse needs of pain assessment. 2012 2013 Total epidurals 41 48 Total PCA morphine 11 17 Total nerve blocks 7 17 Total intra- articular shoulder - LA 3 1 Total 62 82 Clinical practice audit 2012 2013 Patient received a pain assessment as indicated in the protocol? 97% (3% PAPER NOT IN FOLLOW-UP FOLDER) 90% (10% PATIENT PAPER NOT IN FOLDER) Patient was followed up at least 2 times in 24 hours 90% ( Single visit- 4/62; no visit- 2/62) 90% (4/82- single visit; 5/82- no visit) Has a pain assessment tool been utilised? 100% 100% Is there evidence that there were consecutive scores of 7/10 or more? 16% 4.8% Is there evidence of intervention when this has occurred? 100% 100% Is there evidence of consecutive sedation scores of 2 or more? 0 0
- 2. Is there evidence of intervention when this has occurred? N.A N.A Is there evidence of any other reportable observation? Nausea, vomiting, hypotension etc Yes, YES Is there evidence of interventions in response to the other reportable observations? 100% 100% Data entry in pain service sheet Patient name 100% 100% Age 100% 100% Medical problem 95% 100% Name of block 70% 100% File number 92% 100% Premature catheter dislodgement 13%; 7% -epidural;40%- nv.blk, 3.6%; 1.2% epidural;2.4% nv blk Problem area identified in 2012 1. Pain service follow up sheet, not filled and put in the collection box in the recovery 2. High percentage of “2 consecutively high pain scores”. Immediate rescue analgesics are given for high pain score but follow up not done after 30 min, fixed time for rounds, and reliance on ward staff for feedback. Missed cases of analgesia failure. 3. High dislodgement rate 4. Deficient data in the follow up sheets related to name of nerve block and medical problems Solution suggested in 2012 1. Encourage colleagues to fill the chart and put in the collection box, the doctor posted in the recovery, during the morning hours confirms the chart is written. 2. Follow up of patients with high initial pain scores after 30 min to 1 hour. 3. Better fixation, tunneling of catheters 4. Information sessions for colleagues on the importance of filling the charts properly, for example a chart with information about allergies or co morbid conditions will help the pain service in adding co analgesics or rescue medications. Repeat Audit 2013 1. Marked improvement in certain parameters like chart filling up by anesthetists, was observed
- 3. 2. Dislodgement rate decreased due to better fixation 3. Lower pain scores and no cases with high (7/10) pain scores 4. Increase in papers not found in the follow up box. Solution suggested in 2013 Create awareness amongst anesthetist and technician about keeping the paper in the box (better follow up of patients, patient safety and early detection of complication if case followed up). Conducted by Dr Farah Jafri