3. Introduction• The term cirrhosis was first used by Rene Laennec
(1781-1826) to describe the abnormal liver color of
individuals with alcohol induced liver
disease.
• Derived from Greek word Kirrhos means
Yellowish brown color.
Cirrhosis is among the top 10 causes of death in the Western world.
4. Definition
• Cirrhosis is defined as a diffuse (not focal)
involvement of most or all of the liver. It involves the entire liver.
•
process characterised by fibrosisand the
conversion of normal liver architecture into
structurally abnormal nodules containing a mix of
senescent and replicating (often stem/progenitor cell-derived) hepatocytes..
10. Pathogenesis
1. Hepatocellular death
2. Regeneration
3. Progressive fibrosis
4. Vascular reorganization
Three processes are central to the pathogenesis of cirrhosis:
•death of hepatocytes,
•extracellular matrix deposition, and
•vascular reorganization.
11.
12. Pathophsiology :
Liver insult due to alcohol ingestion, viral hepatitis,
exposure to toxin
Hepatocyte damage
Liver inflammation - ↑WBCs, nausea, vomiting, pain,
fever, anorexia, fatigue
Alteration in blood and lymph flow
14. Cont..
• ↓ bile in gastrointestinal tract – light colored stool
• ↑ urobilinogen – Dark Urine
• ↓ vit K absorption- bleeding tendency
• ↓ metabolism of protein, carbohydrate, fats→
hypoglycemia,
• ↓ plasma protein- ascites and edema
• ↓androgen and estrogen detoxification(↓
hormone metabolism)- ↑ estrogen and androgens
hormone – Gynecomastia, loss of body hair,
menstrual dysfunction, spider angioma, palmer
erythema, testicular atrophy
15. Cont..
• ↓ Aldesterone metabolism so ↑ levels – sodium
and water retention-- edema
• Biochemical alteration - ↑ AST, ALT levels, ↑
bilirubin, low serum albumin, prolong prothombin
time, elevated alkaline phosphatase.
• Liver failure
• Hepatic encephalopathy
• Hepatic coma
• Death
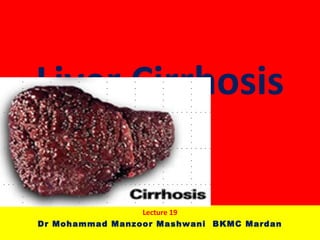
16. Morphology
• Its three main morphologic characteristics are:
• 1.Bridging fibrous septa (delicate fibrous bands/broad scars)
• 2. Parenchymal nodules- micro (<3mm) & macro (>1cm)
• 3. Disruption of the architecture of the entire liver.
4. It occurs following hepatocellular necrosis of varying etiology so that there are
alternate areas of necrosis and regenerative nodules. However, regenerative
nodules are not essential for diagnosis of cirrhosis since biliary cirrhosis and
cirrhosis in haemochromatosis have little regeneration.
17. Clinical manifestations
Early manifestations
• No symptoms
• GI disturbances: anorexia, dyspepsia,
flatulence, weakness, fatigue, nausea,
vomiting, weight loss, abdominal pain,
bloating, diarrhea, constipation
• Abdominal pain, dull and heavy feeling
• Fever, lassitude, weight loss, enlargement of
liver and spleen.
18. Clinical manifestations Cont…
Later manifestations:
Results from liver failure and portal hypertension
• Jaundice
• Peripheral edema
• Ascites
• Others: Skin lesion, hematological disorders,
endocrine disturbances, and peripheral neuropathy
• Advanced stage: small and nodular liver
20. Complications
• The ultimate mechanism of deaths in most
cirrhotic patients is
• (1) progressive liver failure,
• (2) a complication related to portal hypertension,
or
• (3) the development of hepatocellular carcinoma.
21. Complications
Portal hypertension
• The nodules and scar tissue can compress
hepatic veins within the liver.
• This causes the blood pressure within the liver to
be high, a condition known as portal
hypertension.
• Portal venous pressure is more than 15mmHg or
20 cm of water (normal 5-10mm Hg)
22. Cont…
• Is characterized by ↑venous pressure in the portal
circulation, spleenomegaly, large collateral vein,
ascites, systemic hypertension, and esophageal
varices.
• The common area to form collateral channels are in
the lower esophagus( the anastomosis of the left
gastric vein and azygos vein), the parietal
peritoneum, rectum.
• High pressures within blood vessels of the liver
occur in 60% of people who have cirrhosis.
Editor's Notes
Pressure exceeding greater than 22 mm Hg in the portal vein or a pressure difference between the portal vein and the hepatic vein of greater than 12 mm Hg will result in portal hypertension. Measuring portal pressure involves inserting a catheter into the portal vein. The internal jugular, femoral, or medial antecubital vessels are the best way to access the hepatic and portal veins.