Anal cancer video
•Download as PPTX, PDF•
18 likes•17,622 views

1) Anal cancer is uncommon, comprising 2.4% of digestive system cancers in the US, with an estimated 7,060 new cases and 880 deaths in 2013. 2) The median age at diagnosis of anal cancer is 60, younger than the median age of 66 for all cancers. 3) The majority of anal cancers are squamous cell carcinomas caused by HPV infection, while adenocarcinomas are rare. Treatment typically involves chemotherapy and radiation. 4) Five-year survival rates range from 71-78% for early stage anal cancer to 20-24% for late stage or metastatic disease. Combined chemoradiation provides local control in 85-90% of cases.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Anal cancer video
Similar to Anal cancer video (20)
More from Robert J Miller MD
More from Robert J Miller MD (20)
Recently uploaded
Recently uploaded (20)
Anal cancer video
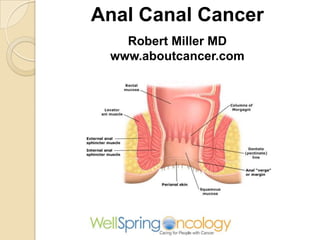
- 1. Anal Canal Cancer Robert Miller MD www.aboutcancer.com
- 2. Incidence of new cases in 2013 Site Men Women Colon 50,090 52,390 Rectum 23,590 16,750 Anus 2,630 4,430 Anal cancer is uncommon. It comprises only 2.4 percent of all digestive system malignancies in the United States
- 3. Age and Anal Cancer US Data 2005 - 2009 • Median age at diagnosis all cancers was 66 for Anus was 60 • Median age at death was 72 for all cancers and for anus was 64 In 2013 estimated 7,060 new cases and 880 deaths so crude death rate was only 12%
- 4. Anal Cancer • This is usually squamous cancer (HPV infection) and is treated with chemo-radiation. • Rectal cancer is adenocarcinoma (from a polyp) and is treated with surgery +/- chemoradiation
- 5. Anal Cancer Rectal bleeding is the most common initial symptom of squamous-cell carcinoma of the anus, occurring in 45 percent of patients. Bleeding from a mass lesion just above the anal sphincter may be ascribed erroneously to the presence of hemorrhoids. Thirty percent of patients have either pain or the sensation of a rectal mass, whereas 20 percent have no rectal symptoms whatsoever
- 6. Histology (what type of cancer from the biopsy and pathology report) Cellular Classification of Anal Cancer Squamous cell (epidermoid) carcinomas make up the majority of all primary cancers of the anus. The important subset of cloacogenic (basaloid transitional cell, non- keratinizing) tumors constitutes the remainder. (about 25%). These two histologic variants are associated with human papillomavirus infection. Adenocarcinomas from anal glands or fistulae formation and melanomas are rare
- 7. Histology Treatment for keratinizing squamous cancers is the same as non- keratinizing (basaloid or cloacogenic
- 8. HPV Cancers Cancers Percent Cervix > 99% Anus 84% Vagina 70% Penis 47% Vulva 44% Oropharynx 36% Oral Cavity 24% JCO May 2011;29:1785
- 9. HPV Cancers 2004-2008 Cancer All Cases HPV Caused Cervix 11,967 11,500 Vulva 3,136 1,600 Vagina 729 500 Penis 1,046 400 Anus (female) Anus (male) 2,900 1,678 2,700 1,600 Oropharynx (female) 2,370 1,500 Oropharynx (male) 9,356 5,900
- 10. HPV Types
- 11. Prevalence of High Risk HPV infection found in biopsy Anus cancer: 84% Rectal cancer: 0 % N Eng J Med 1997;337:1350
- 12. The proximal end of the anal canal begins anatomically at the junction of the puborectalis portion of the levator ani muscle and the external anal sphincter, and extends distally to the anal verge, a distance of approximately 4 cm. The anal canal is divided by the dentate line, which overlies the transition from glandular (columnar) to squamous mucosa that is often referred to as the transitional zone. Anal Canal lower 4cm tumors are classified as rectal cancers if their epicenter is located more than 2 cm proximal to the dentate line or proximal to the anorectal ring on digital examination, and as anal canal cancers if their epicenter is 2 cm or less from the dentate line
- 13. Anal Canal and Anal Margin
- 15. Pelvic Anatomy (female) colon Anal canal bowel uterus rectum bladder
- 16. Pelvic Anatomy (male) Anal canal
- 17. Lymph Nodes at Risk in Anal Cancer • Cancers from the distal region (below dentate line) go to superficial groin (inguinal) nodes • Cancers that arise ate or proximal (above) the dentate line are directed to anorectal, perirectal, paravetebral and
- 18. para-aortic peri-rectal inguina l pelvic inguinal Lymph Nodes at Risk in Anal Cancer
- 19. Stage Start with Tumor (T) stage
- 20. Stage Then Nodes (N) or Metastases (M)
- 21. Stage Then combine T, N, M
- 22. Cancer Imaging for Anal Cancer in a study of 61 patients with anal cancer the sensitivity for nodal regional disease by PET versus conventional imaging (CT and/or MRI) was 89 and 62 percent, respectively
- 23. CT scan = large anal cancer
- 24. Since cancers use more glucose than normal cells (hypermetabolic) they will ‘light up’ on a PET Scan
- 25. CT and PET Imaging for Anal Cancer
- 26. PET scan showing small anal cancer
- 28. PET and Lymph Node Metastases
- 29. PET and Lymph Node Metastases
- 30. More advanced case of anal cancer that has spread on PET scan to para- aortic lymph nodes PET and Lymph Node Metastases
- 34. Treatment of Anal Cancer • Anal canal Stages I – III : radiation + chemotherapy (5FU + Mitomycin) • Anal margin Stage I : wide local excision • Anal margin Stage II – III: radiation + chemotherapy (5FU + Mitomycin) • Stage IV: Cisplatin based chemotherapy +/- radiation
- 35. CT scan is obtained at the time of simulation CT images are then imported into the treatment planning computer
- 36. In the simulation process the CT and PET scan images are used to create a computer plan
- 37. Computer generated images of anal cancer
- 39. Tomotherapy for anal cancer, high dose to anus and groin nodes, while avoiding the bladder and femurs
- 40. Radiation Dose and Technique • Radiation is daily, Monday through Friday for 5 to 6 weeks • Radiation works best when combined with chemotherapy • Minimal dose of 45Gy (1.8Gy X 25) up to 54 to 59Gy for more advanced cancers • The radiation should include the lymph node regions for at least part of the treatment
- 42. Target Volumes for Anal Carcinoma For RTOG 0529 Radiation Dose and Techniqu e
- 43. RTOG 0529: A Phase 2 Evaluation of Dose-Painted Intensity Modulated Radiation Therapy in Combination With 5-Fluorouracil and Mitomycin-C for the Reduction of Acute Morbidity in Carcinoma of the Anal Canal DP-IMRT was associated with significant sparing of acute grade 2+ hematologic and grade 3+ dermatologic and gastrointestinal toxicity. IJROBP 2013;86:27 Anus cancer Nodes High Risk Node
- 44. Side Effects of Pelvic Radiation Radiation fields Radiation may hit the small bowel causing some cramps, diarrhea and fatigue High dose area
- 45. Side Effects of Pelvic Radiation Radiation fields Radiation may hit the bladder and rectum causing urinary burning or frequency and ano- rectal irritation and skin burning High dose area In pre-menopausal women, radiation is likely to effect ovarian function and should not be used if the woman is pregnant
- 46. Results with combined chemo- radiation for anal cancer • Local failure rates of 14 to 37 percent • Five-year overall survival rates of 72 to 89 percent • Five-year colostomy-free survival rates of 70 to 86 percent
- 47. Long-Term Update of US GI Intergroup RTOG 98-11 Phase III Trial for Anal Carcinoma JCO December 10, 2012 vol. 30 no. 35 4344-4351 Survival 78% 71%
- 48. 5 Year Survival with Anal Cancer Stage Squamous Non- squamous I 71.4 59.2 II 63.5 52.9 IIIA 48.1 37.7 IIIB 43.2 24.4 IV 20.9 7.4 NCDB 1998-99, n = 3598
- 49. 5 Year Survival with Anal Cancer NCDB 1985 - 2000 Stage Survival I 70% II 59% III 41% IV 19%
- 50. 5 Year Survival with Anal Cancer (SEER Data Base) SEER 1999-2006 Stage Incidence Survival Local 50% 80% Regional 29% 60% Distant 12% 30.5%
- 51. Fluorouracil, mitomycin, and radiotherapy vs fluorouracil, cisplatin, and radiotherapy for carcinoma of the anal canal: a randomized controlled trial. US Gastrointestinal Intergroup trial RTOG 98-11, The 5-year overall survival rate was 75% in the mitomycin-based group and 70% in the cisplatin- based group. The 5-year local-regional recurrence and distant metastasis rates were 25% and 15%, respectively, for mitomycin-based treatment and 33% and 19%, respectively, for cisplatin-based treatment. The cumulative rate of colostomy was significantly better for mitomycin-based than cisplatin-based treatment (10% vs 19%) JAMA. 2008 Apr 23;299(16):1914-21.
- 52. Survival by Stage in a series of 270 patients with anal cancer 5 Year Survival by Stage T1: 86% N0: 76% T2: 86% N1: 54% T3: 60% T4: 45%
- 53. Odds of Requiring a Colostomy • In large series the odds were 10 to 30% • 235 patients diagnosed with anal cancer between 1995 and 2003 the five-year cumulative incidences of tumor-related and treatment related colostomy were 26 and 8 percent, respectively. Large tumor size (>6 cm) was associated with a higher risk of tumor-related colostomy, while a history of prior excision was a risk factor for therapy-related colostomy. • RTOG trial 98-11 five-year colostomy rates among patients treated initially with Chemoradiotherapy were 9 percent for those with node-positive disease, and 19 percent for tumors >5 cm in diameter, regardless of nodal status. Overall, 78 percent of the colostomies were performed for persistent or recurrent disease.
- 54. Anal Cancer Robert Miller MD www.aboutcancer.com