Texas Tales Brenham and Amarillo Experiences Elevated by Find American Rental...
Mastoidectomy Epitympanum
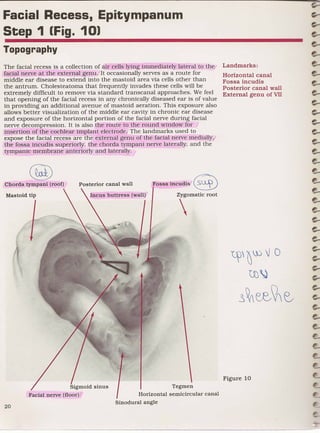
1. Facial Recess, Epitympanum
Step 1 (Fig. 10)
Topography
Landmarks:
The facial recess is a collection of air cells lying immediately lateral to tho/'
facial nerve at the external genu. It occasionally serves as a route for Horizontal canal
middle ear disease to extend into the mastoid area via cells other than Fossa incudis
the antrum. Cholesteatoma that frequently invades these cells will be Posterior canal wall
extremely difficult to remove via standard trans canal approaches. We feel External genu of VII
that opening of the facial recess in any chronically diseased ear is of value
in providing an additional avenue of mastoid aeration. This exposure also
allows better visualization of the middle ear cavity in chronic ear disease
and exposure of the horizontal portion of the facial nerve during facial
nerve decompression. It is also the route to the round window for I
insertion of the cochlear implant electrode! The landmarks used to
expose the facial recess are the external genu of the facial nerve mediallyI
the fossa incudis superiorly, the chorda tympani nerve laterally, and the
tympanic membrane anteriorly and laterally./
@
§)
Posterior canal wall Fossa incudis
Chorda tympani (roof)
Incus buttress (wall) Zygomatic root
'l? ~})i 0
UJ~
~~ee~~
Tegmen
Sigmoid sinus
Horizontal semicircular canal
Facial nerve (floor)
Sinodural angle
2. Step 2 [Fig. 11):
Opening the Facial Recess
One begins dissection of the facial recess by identifying the external genu Landmarks:
or the'descending portion of the facial nerve in the mastoid cavity. As
Posterior canal wall
preViously indicated, a free flow of irrigating fluid is used to allow clear
Horizontal canal
and constant visualization of the underlying bone so that color variations
Fossa incudis
in it may be easily identified. The microscope is turned to 10 power. The
Facial recess cells (if
color of the facial nerve is pearly white in the preserved bone and pinkish
present)
(from the vascularity of the facial canal and the nerve sheath) in a living
External genu
specimen. Generally, this dissection is accomplished with a cutting burr_
until a change in bone character is identified; further dissection is
performed with a diamond burr. A thin layer of bone is preserved over the
facial nerve and, because color changes in the bone will occur before the
facial sheath is uncovered, the soft tissue is not injured.
Identification of a facial recess cell tract is often possible by thinning the
posterior canal wall enough to see the shadow of an instrument through
the bone. One must not perforate the canal wall, disrupt the chorda
tympani, or transect the annulus.
Zygomatic root
Posterior canal wall
Mastoid tip Incus
I
Sigmoid sinus
3. Step 3 (Fig. 12):
Completing the Recess
With the new landmark of the facial sheath, the nerve is skeletonized Landmarks:
distally along its descending portion in the mastoid and then medially as
Facial nerve
it follows the floor of the facial recess into the middle ear space. Smaller
Incus
burrs will be necessary to accomplish most of the dissection in the facial
Fossa incudis
recess since the recess itself rarely exceeds two or three millimeters.
Chorda tympani
Inferiorly the chorda tympani nerve is detected as it leaves the facial
Stapes
nerve. Dissection does not sacrifice this structure. The chorda tympani
Horizontal canal
nerve joins with the tympanic membrane anteriorly and laterally at the
annular edge; thus, following the chorda tympani generally prevents
disruption of the tympanic membrane.
Long process of incus
V
Buttress )
Chorda tympani ~~VJ ~
Descending segment of facial nerve
1 Stapes Tegmen
Digastric mu::'e
Horizontal semicircular canal
External genu
Sigmoid sinus
4. Step 4 (Fig. 13):
The Middle Ear Through the Facial Recess
With the facial recess fully opened, one can easily visualize the horizontal Landmarks:
portion of the facial nerve, the lenticular process of the incus, the
Facial nerve
incudostapedial joint, the capitulum of the stapes, the stapedial tendon,
Incus
and, with proper angulation, the cochleariform process.
Lenticular process
Incudostapedial joint
The round window may be easily identified inferior to the stapedial
Stapes
landmarks. Superiorly, a buttress of bone is preserved between the short
Round window
process of the incus and the facial recess. This is commonly termed quot;the
Cochleariform process
buttress.quot; Drilling through the buttress causes disruption of the
Chorda tympani
ligaments to the short process of the incus and incudal dislocation is a /
Horizontal canal
possibility ..
Posterior canal wall
!
Promontory External genu
Pyramidal process .
5. Step 7 (Fig. 16):
Exposure of the Anterior Epitympanum
Landmarks:
After removal of the head of the malleus and body of the incus, this
dissection allows unimpeded inspection of all epitympanic areas. In a well
Stapes
pneumatized bone, air cells extending anteriorly into the petrous apex
Facial nerve
may also be seen.
Cochleariform process
Long process of malleus
The figure shows the expansive exposure obtained with this technique.
Eustachian tube
Note the cog. a bony ledge extending into the epitympanum from the
Cog
tegmen anterior to the amputated head of the malleus. This spicule may
separate the epitympanum into posterior and anterior compartments.
Removal of cholesteatoma that is harbored anteriorly, which is common,
requires careful burring away of the cog.
Cochleariform process Zygomatic root
Chorda tympani
I
Hypotympanum Tegmen
Horizontal semicircular canal
Peritubular cells
Facial nerve
Promontory
Eustachian tube Canal of tensor tympani
Pyramidal process