Emergency procedures summary
•
2 likes•1,557 views

1) The document outlines several emergency procedures including rapid sequence intubation, chest tube insertion, femoral line insertion, CVP line insertion, and peritoneal tap. 2) It provides detailed steps for each procedure including necessary equipment, patient positioning, anesthesia, insertion technique, and post-procedure care. 3) The procedures are commonly assessed in OSCE exams and require careful preparation, sterile technique, knowledge of anatomy, and verification of correct placement.

Recommended
More Related Content
Viewers also liked
Viewers also liked (20)
Similar to Emergency procedures summary
Similar to Emergency procedures summary (20)
More from Dr. Rubz
More from Dr. Rubz (20)
Emergency procedures summary
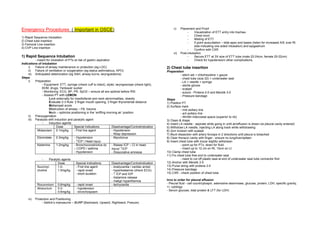
- 1. Emergency Procedures ( Important in OSCE) v) Placement and Proof - Visualization of ETT entry into trachea - Chest movt 1) Rapid Sequence Intubation - Misting of ETT 2) Chest tube insertion - 5 point auscultation – bilat apex and bases (listen for increased A/E over Rt 3) Femoral Line insertion side indicating one sided intubation) and epigastrium 4) CVP Line insertion - Confirm with CXR vi) Post-intubation 1) Rapid Sequence Intubation - Secure ETT at 3X size of ETT tube (male 22-24cm, female 20-22cm) - meant for intubation of PTs at risk of gastric aspiration - Check for hypotension/ other complications Indications of intubation i) Failure of airway maintenance or protection (eg LOC) 2) Chest tube insertion ii) Failure of ventilation or oxygenation (eg status asthmaticus, APO) Preparation iii) Anticipated deterioration (eg SAH, airway burns, laryngoedema) - stitch set + chlorhexidine + gauze Steps - chest tube (size 22) + underwater seal i) Preparation - LA + needle + syringe - Equipment: ETT, syringe (check cuff is intact), stylet, laryngoscope (check light), - sterile gloves BVM, drugs, Yankauer sucker - scalpel - Monitoring: ECG, BP, PR, SpO2 – ensure all are optimal before RSI - suture - Prolene 2-0 and Mersilk 3-0 - Assess PT with LEMON: - Pressure bandage Look externally for maxillofacial and neck abnormalities, obesity Steps Evaluate 2-3 Rule: 2 finger mouth opening, 3 finger thyromental distance 1) Position PT Mallampati score 2) Surface mark Obstruction of airway – FB, trauma - mid axillary line Neck – optimize positioning in the ‘sniffing morning air’ position - ant axillary line ii) Preoxygenation - 4th/5th intercostal space (superior to rib) iii) Paralysis with induction and paralytic agent 3) Clean & drape - Induction agents 4) Insert LA needle - aspirate while going in until air/effusion is drawn (ie pleural cavity entered) Dose Special Indications Disadvantage/ContraIndication 5) Withdraw LA needle, injecting LA along track while withdrawing Midazolam 0.1mg/kg - First line agent - Hypotension 6) 2cm incision with scalpel - Resp depression 7) Blunt dissection with artery forceps in 2 directions until pleura is breached Etiomidate 0.3mg/kg - Hypotension - Myoclonus 8) Clear thoracic cavity with finger - ensure no lung/liver/spleen - ↑ICP / Head injury 9) Insert chest tube with trocar slightly withdrawn Ketamine 1-2mg/kg - Bronchoconstrictive dz - Raises ICP – CI in head - point up for PTx, down for fluid. – COPD / asthma injury/ ↑ICP - Insert up to 12 cm on Rt, 10cm on Lt - Hypotension - Dissociative amnesia 10) Clamp chest tube 11) Fix chest tube free end to underwater seal - Paralytic agents - need to cut off plastic seal at end of underwater seal tube connector first Dose Special Indications Disadvantage/ContraIndication 12) Anchor with Mersilk 3-0 Succinyl- 1.0- - First line agent - bradycardia / cardiac arrest 13) Purse string with prolene 2-0 choline 1.5mg/kg - rapid onset - hyperkalaemia (check ECG) 14) Pressure bandage - short duration - ↑ ICP and IOP 15) CXR - check position of chest tube - histamine release - malign hyperthermia Invx to order for pleural effusion Rocuronium 0.6mg/kg - rapid onset - tachycardia - Pleural fluid - cell count/cytospin, adenosine deaminase, glucose, protein, LDH, specific gravity, +/- cytology Atracurium 0.3- - hypotension - 0.6mg/kg - bronchospasm - Serum glucose, total protein & LFT (for LDH) iv) Protection and Positioning - Sellick’s manoeuvre – BURP (Backward, Upward, Rightward, Presure)
- 2. 3) Femoral line 4) CVP line Preparation Preparation - Seldinger femoral line set (length 19.5cm for femoral line, 14cm for IJ line) - Seldinger CVP line set - 21G green needle - 21G green needle - Syringe + saline flush - Syringe + saline flush - Stitch set - Syringe for taking blood if required - LA + needle + syringe - Stitch set - Sterile gloves - LA + needle + syringe - Scalpel - Sterile gloves - Suture – prolene - Scalpel - Bandage - Suture – prolene Steps - Opsite dressing 1) Landmark - locate femoral pulse along inguinal fold, 2-3cm inf & 1cm medial to pubic tubercle Steps 2) Prepare Seldinger set 1) Surface mark - flush catheter ports x2 - Position PT - Trendelenberg position w head rotated to left - free guidewire - apex btwn med & lat heads of Rt SCM towards Rt nipple / Medial corner of triangle - attach green needle (21G) to searching syringe, half-fill syringe with sterile water formed by heads of SCM towards Lt nipple - prepare scalpel, stitch set and sutures for anchoring stitch 2) Prepare CVP line set - prepare bandage - Flush & lock all 3 ports - prepare LA and needle - Withdraw hooked tip of guide wire just into cap - additional syringe and saline for aspiration of catheter ports - Withdraw 2ml N/S into locating syringe & affix needle 3) Clean & drape 3) Clean & drape 4) Apply LA 4) LA at apex of triangle of SCM heads 5) Search for femoral vein with induction syringe provided in Seldinger set (just medial to femoral 5) Insert locating needle while applying suction at 45degrees. Aim for Rt nipple. Carotid artery artery) should be medial to IJV. - insert at 45degree angle along course of femoral vein while aspirating until flash back 6) Stop when flashback occurs. occurs when needle hits vein - Stop suction & watch. Ensure no arterial pulsation of blood into syringe. 6) Ensure flash back is NON-PULSATILE 7) Remove Syringe, block needle w thumb - if so, femoral artery was entered. Remove and apply pressure. 8) Insert guide wire 7) Remove syringe and cover needle with thumb 9) Remove needle 8) Insert guide wire 10) Small incision w scalpel at point of CVP insertion - always ensure a good length of wire is left externally. Consider applying artery forceps 11) Insert dilator over wire & remove to wire end to prevent loss of wire. 12) Insert CVP line over wire up to 10-12cm. 9) Remove induction needle over wire 13) Check backflow is good 10) Make small incision in the skin at the base of the wire with scalpel 14) Check CVP (normal 8-16cmH2O) – assistant to attach manometer device to 3 way tap and 11) Thread dilators over guide wire in succession, starting from smallest to biggest saline drip 12) Thread femoral catheter over guide wire 15) Flush ports 13) Remove guide wire 16) Anchor CVP line w suture 14) Check each port for flash back 17) Opsite dressing over CVP line - attach syringe to port, release clamp, aspirate for good easy flow of venous blood, 18) CXR - tip of CVP line should be at level of carina. Ensure no PTx flush with saline, then clamp and seal 15) Anchor with sutures 16) Cover catheter ports with sterile gauze, bandage 17) Document
- 3. 5) Peritoneal Tap Steps Surface mark - LIF / RIF, percuss for fluid level and ensure no organomegaly 1) Clean & Drape 2) LA - blue needle, insert with suction until peritoneal fluid is drawn, then withdraw needle and give lignocaine along track 3) Prepare Saldinger set - unhook J tip 4) Insert 20 ml syringe with introducing needle until peritoneal fluid is withdrawn freely - draw 20mls for investigations 5) Remove syringe from needle and cover needle with fingertip 6) Insert guidewire and ensure no resistance is met 7) Remove needle over guide wire 8) Nick skin with scalpel 9) Progressively dilate track with introducers over guide wire 10) Insert pigtail over guidewire 11) Remove guidewire 12) Fix tap on end of pigtail, ensuring tap is closed 13) Place plastic flange around pigtail and secure with cable tie 14) Connect urine bag to tap 15) Tape down with elastic bandages 16) Document 17) Drain up to 6L/Day with IV alb cover Digitally signed by DR WANA HLA SHWE DN: cn=DR WANA HLA SHWE, c=MY, o=UCSI University, School of Medicine, KT-Campus, Terengganu, ou=Internal Medicine Group, email=wunna. hlashwe@gmail.com Reason: This document is for UCSI year 4 students. Date: 2009.02.24 10:00:43 +08'00'