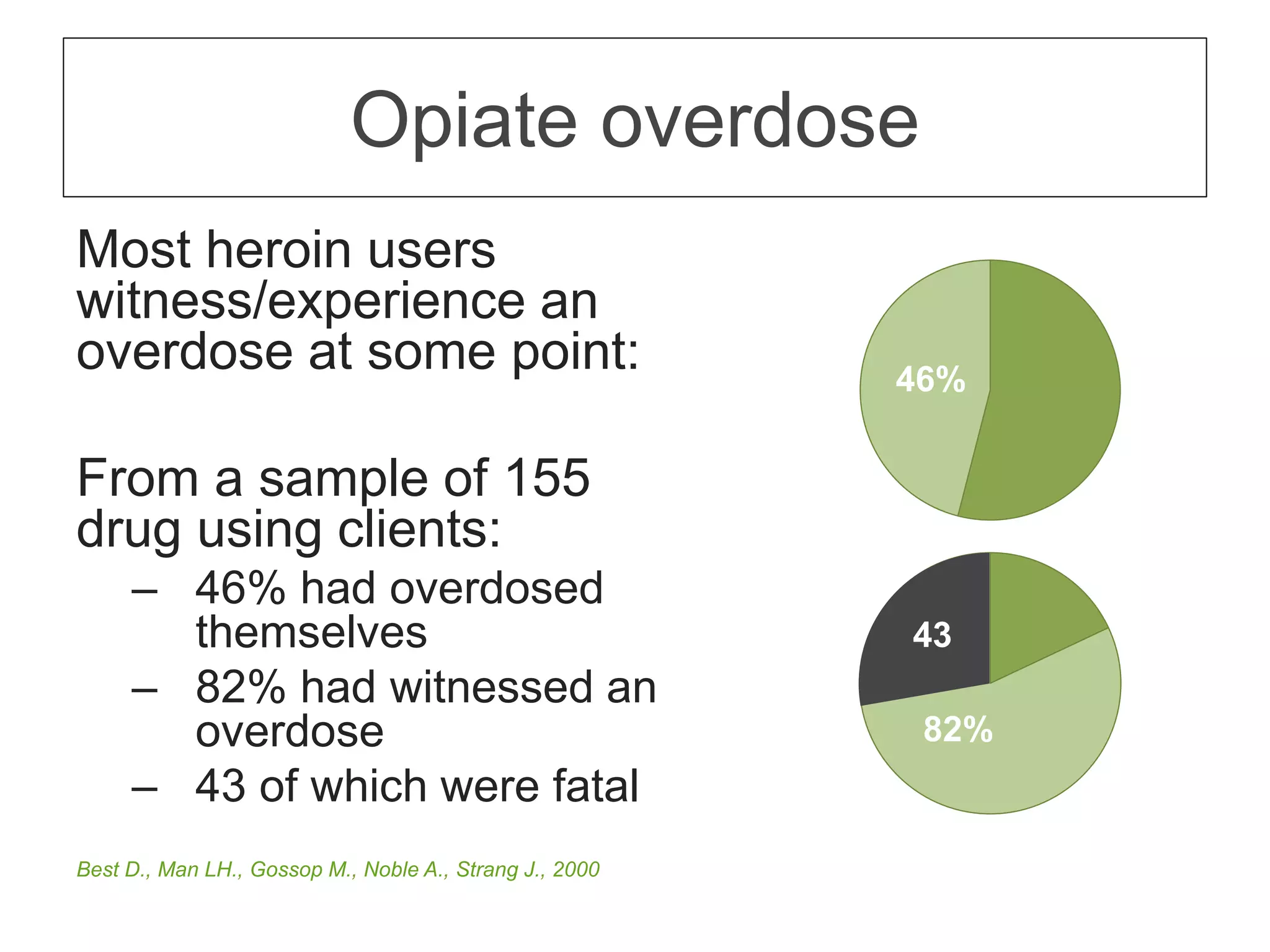
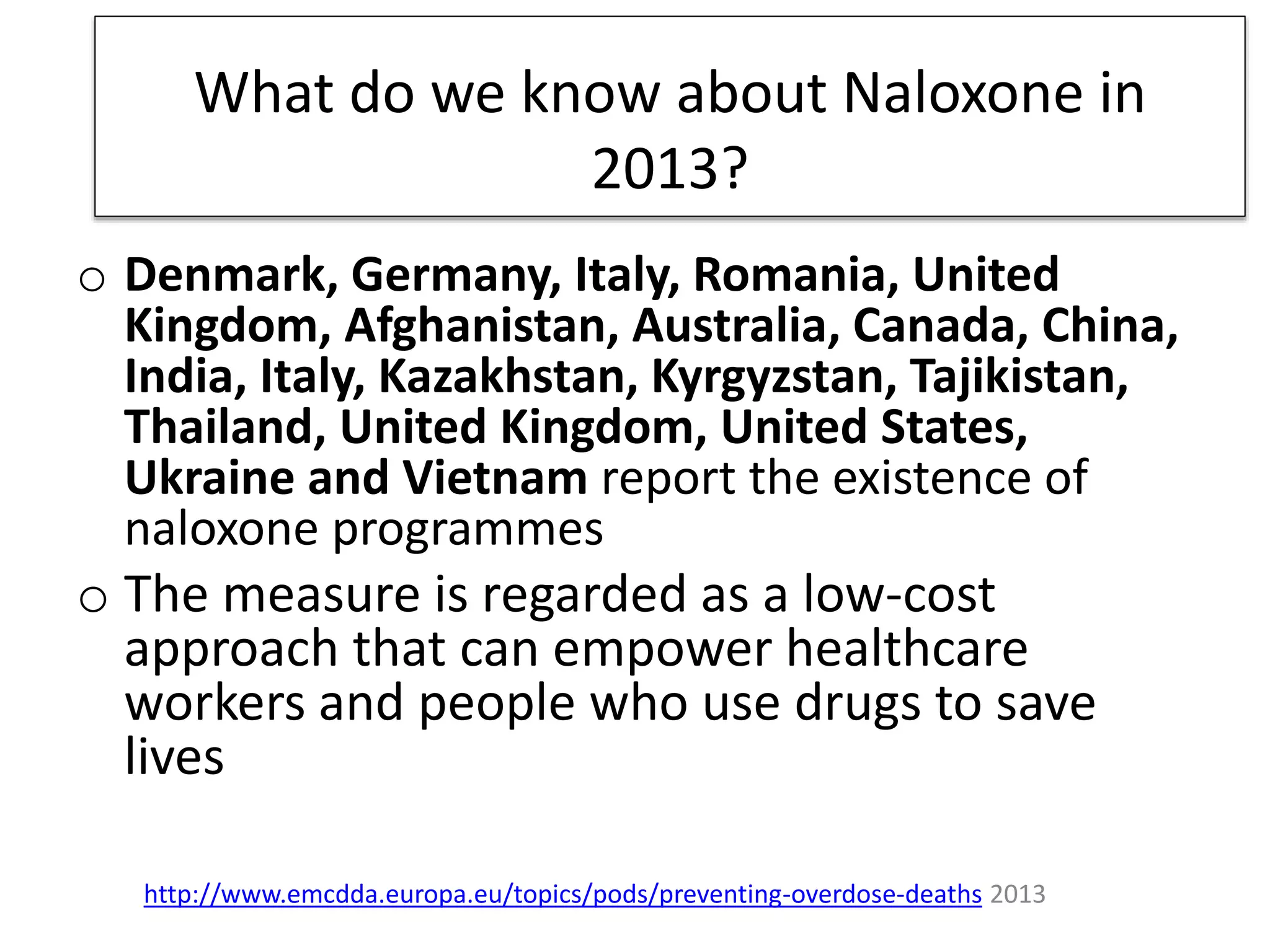
The document discusses the importance of naloxone as a lifesaving intervention for opioid overdoses, noting that it is underutilized despite its effectiveness. It highlights alarming statistics on opioid use and overdose deaths while calling for broader access to naloxone and changes in policy to mitigate these issues. The text emphasizes the need for awareness and understanding among healthcare providers and the public regarding naloxone's benefits.