Medical release hippa_form_new
•
0 likes•131 views

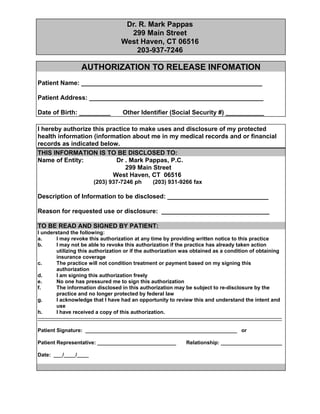
This document is an authorization form for Dr. R. Mark Pappas to release a patient's protected health information. It lists the patient's name and address, date of birth, and social security number. It authorizes Dr. Pappas to disclose the patient's medical and financial records to Dr. Pappas' own practice located in West Haven, Connecticut. The patient must sign to acknowledge they understand their rights regarding the authorization and that they are signing freely.

Recommended
More Related Content
What's hot
What's hot (14)
Similar to Medical release hippa_form_new
Similar to Medical release hippa_form_new (20)
More from Wendy Cahill
Medical release hippa_form_new
- 1. Dr. R. Mark Pappas 299 Main Street West Haven, CT 06516 203-937-7246 AUTHORIZATION TO RELEASE INFOMATION Patient Name: ____________________________________________________ Patient Address: __________________________________________________ Date of Birth: _________ Other Identifier (Social Security #) ___________ I hereby authorize this practice to make uses and disclosure of my protected health information (information about me in my medical records and or financial records as indicated below. THIS INFORMATION IS TO BE DISCLOSED TO: Name of Entity: Dr . Mark Pappas, P.C. 299 Main Street West Haven, CT 06516 (203) 937-7246 ph (203) 931-9266 fax Description of Information to be disclosed: _____________________________ Reason for requested use or disclosure: _______________________________ TO BE READ AND SIGNED BY PATIENT: I understand the following: a. I may revoke this authorization at any time by providing written notice to this practice b. I may not be able to revoke this authorization if the practice has already taken action utilizing this authorization or if the authorization was obtained as a condition of obtaining insurance coverage c. The practice will not condition treatment or payment based on my signing this authorization d. I am signing this authorization freely e. No one has pressured me to sign this authorization f. The information disclosed in this authorization may be subject to re-disclosure by the practice and no longer protected by federal law g. I acknowledge that I have had an opportunity to review this and understand the intent and use h. I have received a copy of this authorization. ------------------------------------------------------------------------------------------------------------------------------------------Patient Signature: ____________________________________________________ or Patient Representative: ___________________________ Date: ___/____/____ Relationship: _____________________