
Recommended
More Related Content
Similar to chiasmal syndrome.pptx
Similar to chiasmal syndrome.pptx (20)
Recently uploaded
Recently uploaded (20)
chiasmal syndrome.pptx
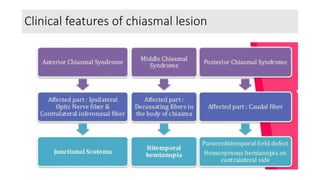
- 1. Clinical features of chiasmal lesion
- 2. Chiasmal syndrome- Pathophysiology • Most chiasmal syndromes result from: Neoplastic disorders Developmental derangements Radiation injury Inflammation, infection, infarction Demyelination Transection, or hypoplasia The hallmark of chiasmal disease is a bitemporal hemianopia. Some form of visual field testing is essential. Inferior lesions have to grow large and compress the lower nasal fibers first and tend to give an upper bitemporal field defect. Lesions from above tend to cause an inferior defect.
- 3. Chiasmal syndrome- Pathophysiology • In young children, chiasmal disease often presents late because the child compensates and is not suspected of having poor vision until there is substantial bilateral visual loss • There is often an acuity defect. Chiasm splitting lesions, such as trauma, do not affect acuity greatly because the nasal field and the nasal half of the fovea is not affected, but involvement of the optic nerve or widespread involvement of both crossed and uncrossed fibers in the chiasm give rise to an acuity defect. • Frequently, one eye has a very severe acuity defect and the other is relatively spared, except for a field defect. • In chronic lesions, there is often preservation of a high level of acuity despite funduscopic evidence of a profound loss of neurons. • With optic nerve involvement there is significant color vision defect. Stereoacuity tests and Bagolini striated lens are useful tests in patients with suspected chiasmal compression. • Decreased stereoacuity is common with chiasmal lesions, even when no visual field abnormalities are detectable. Stereopsis can be elicited with complete chiasmal transection by haploscopic stimulation of the intact temporal retinas. • This shows the sensory capacity for stereopsis is retained in chiasmal transection but the absence of motor fusion precludes stereopsis. Bagolini striated lens testing reveals a binocular “mountain” pattern in chiasmal lesions. • Children with early-onset chiasmal disease may present with nystagmus. The classic form is see-saw nystagmus, but most patients have a compound nystagmus with vertical, horizontal, and rotary components
- 4. Optic atrophy frequently occurs in chiasmal disease. There may be a generalized loss of neurons, or a pattern of band atrophy due to the loss of the fibers subserving the temporal fields and the preservation of fibers subserving the intact nasal field Congenital suprasellar tumors can produce horizontal “bow-tie” cupping with selective loss of the nasal and temporal nerve fiber layer. Papilledema in these optic discs occurs predominantly in the superior and inferior poles In bitemporal hemianopia the hemifield slide phenomenon may occur . Since only the nasal portion of each visual field is functioning fully, corresponding retinal points between the two eyes no longer exist. Sensory fusion becomes impossible, and motor fusion cannot maintain alignment. A previous heterophoria becomes a manifest deviation. Esodeviations lead to letters or words appearing deleted or duplicated. A vertical hemifield slide causes the child to lose track of which line of text they are reading. These children do not complain of diplopia but rather a duplication of the middle of words or objects. The hemifield slide phenomenon does not require a complete bitemporal hemianopia and can occur as the initial symptom . Rarely, chiasmal tumors can produce photophobia as their presenting symptom.
- 5. Evaluation Complete ophthalmic history, endocrine history, and eye exam with attention to visual acuity, color vision, pupils, and ophthalmoscopy. Check visual fields with attention to vertical midline. Head and orbital CT scan in emergencies or suspect pituitary apoplexy. Orbit and brain MRI with and without contrast. Lab tests: Consider checking hormone levels.