
Recommended
More Related Content
What's hot
What's hot (18)
Similar to Pharmacotherapy of arrythmias
Similar to Pharmacotherapy of arrythmias (20)
More from tolcha regasa
More from tolcha regasa (6)
Recently uploaded
Recently uploaded (20)
Pharmacotherapy of arrythmias
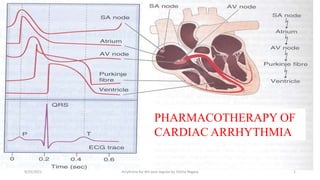
- 1. Pharmacotherapy of arrhythmias 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 1 PHARMACOTHERAPY OF CARDIAC ARRHYTHMIA
- 2. Normal Cardiac Cycle Systole Diastole Electrical Depolarization “activate” Repolarization “recovery” Mechanical Contract “empty” Relax “fill” 2 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa
- 3. Conducting system vs contractile tissue of the heart • Normal heart rate • Action potential • ECG 3 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa
- 4. Conducting system vs contractile tissue of the heart 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 4 Conducting System of the Heart: Impulse Propagation: SA node AV-node Bundle of His Purkinje fibers ventricle. SA node is the initial pacemaker. SA node, AV node, Purkinj fibers Atrial & Ventricular muscles Contractile tissue of the heart
- 5. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 5
- 6. 1. Resting membrane potential (RMP) • In resting state: • Myocytes are permeable to K+ only. • RMP determined by K+ conc. (Ko & Ki). • Ki is 150 mmol/L and Ko 4 mmol/L. • Resting membrane potential ranges: • From – 80 to -90 mv in contractile cells • From -60 to -70 mv in pacemaker cells (SA node, AV node and His- Purkinj fibers) . • Phase 4 of AP represents RMP. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 6
- 7. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 7
- 8. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 8 2. Cardiac Action Potential Na+ Ca++ K+ Na+ K+
- 9. 9 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa
- 10. Potential Terms 1. Refractory Period (RP): Phases 1,2 & 3. • ERP (absolute refractory period): • Phases 1 & 2 represent ERP (no response to any stimuli). • RRP (Relative Refractory Period): • Phase 3 represents RRP (respone only to strong stimuli. 2. Action Potential Duration: Phases 1,2 & 3: - During APD, the heart in refractory state and no impulse propagation. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 10
- 11. Potential Terms 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 11 APD ERP RRP Relative Refractory Period Effective Refractory Period Action Potential Duration
- 12. Definitions of Arrhythmias & antiarrhythmics • Arrhythmias or dysrhythmias: Disturbances in cardiac rhythm (rate and/or regularity) due to abnormality in impulse origination (ectopic beats) or abnormality in conductivity (reentry) or both. • Antidysrhythmic drugs: Drugs which suppress abnormalities of automaticity and/or conductivity by blocking specific ion channels (Na+, Ca++ and K+) or by altering autonomic functions. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 12
- 13. Causes of Cardiac Arrhythmias • Electrolyte disturbances: hypokalemia, hyperkalemia). • Cardiac ischemia & MI: e.g., hypoxia O2 supply. • Structural damage: changing the conduction pathway. • Drug toxicity:: e.g., digitalis toxicity. • Autonomic changes: sympathetic or vagal tone. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 13
- 14. Mechanisms of Arrhythmias Genesis A. Abnormal automaticity: Altered normal automaticity. Ectopic beats Triggered automaticity. B. Abnormal conductivity Re-entry Heart block 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 14
- 15. 1) Abnormal Automaticity a) Alteration of Normal Automaticity • In pacemaker cells (SA, AV & H-P fibers. • Precipitated by: • Autonomic disturbance: • Sympathetic activity sinus & nodal tachycardia. • vagal tone sinus bradycardia. • Hypokalemia sinus tachycardia. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 15
- 16. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 16 Impulses originate at SA node but at a slow rate e.g. of Abnormality of Impulse Generation
- 17. b) Abnormal Ectopic Pacemakers • Non pacemaker cells act as pacemaker due to formation of ectopic foci . e.g., atrial or ventricular cells. • Inward K+ & Ca++ currents may be involved in the genesis of this type of arrhythmia. • Atrial or ventricular extr-asystoles are the result. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 17
- 18. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 18 - Impulses originate at ectopic pacemaker - QRS is wider than normal and distorted in Shape. Usually no P wave
- 19. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 19 - Impulses originate at ectopic pacemaker - P wave is slighly different from normal sinus beat - PR interval is often long and QRS is narrow.
- 20. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 20 It is a secondary depolarization that occurs before complete repolarization
- 21. c) Triggered Arrhythmias • Triggered Automaticity (after depolarization): • Triggered arrhythmias = persistent abnormal automaticity. • Two types: 1. Early after depolarization: • Secondary depolarization during phase 3 repolarization i.e., secondary depolarization before complete repolarization. 1. Delayed after-depolarization:. • Secondary depolarization after complete repolarization but during phase 4. • Caused by Ca++ overload caused by: • Catecholamines • Digitalis • Cardiac ischemia.. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 21
- 22. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 22 It is a secondary depolarization that occurs just after complete repolarization
- 23. 2. Abnormality in Conductivity in Purkinj Fibers (Re-entry) 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 23
- 24. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 24
- 25. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 25
- 26. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 26
- 27. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 27
- 28. Re-entry & Wolf-Parkinson White Syndrome • Impulse originates in SA node BUT pass in accessory pathway anterogradely not in AV node, so pass rapidly. • The conducted impulses then travel retrogradely through the AVN, re-exciting the atria causing atrial arrhythmias. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 28
- 29. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 29
- 30. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 30
- 31. Types of Cardiac Arrhythmias A) Supraventricular arrhythmias: • Sinus tachycardia 90 beats min. • Sinus bradycardia 60 beats min. • Premature atrial contractions (PACs) • Atrial tachycardia (regular pulse; up to 200 beats min). • Atrial flutter (regular pulse; 200-300 beats min). • Atrial fibrillation (irregular pulse; 300 beats min). • Nodal tachycardia (AV nodal reentry; a common type of [SVT]). B) Ventricular Arrhythmias: • Premature ventricular contractions (PVCs), • Ventricular tachycardia (VT), • Ventricular fibrillation (VF), • Bundle branch block, • Torsade de pointes. N.B. Ventricular arrhythmias are life-threatening arrhythmias. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 31
- 32. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 32 Classes Examples Class I: Na –channel blockers I A Quinidine, Procainamide (IV), Disopyramide I B Lidocaine, phenytoin, Mexiletine IC Flecainide, Propafenone Class II: -blockers Propranolol, sotalol, esmolol Class III: K+-channel blockers Amiodarone, Dofetilide, Sotalol, Ibutilide Class IV: Ca2+-channel blockers Verapamil, diltiazem Class V: Miscellaneous Adenosin, digoxin & Magnesium Vaughan-Williams Classification Arbitrary classification (not absolute): e.g., quinidine has class I and class III effects e.g., Sotalol has class II and class III effects.
- 33. Mechanism of action of class I 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 33
- 34. SUPRAVENTRICULAR ARRHYTHMIAS: Sinus Bradycardia • Sinus bradycardia, originating in the SA node, is defined by a sinus rate less than 60 beats/min • Can occur in those involved in vigorous activity: eg. Athletes • Idiopathic ( sick sinus syndrome) in advanced age - The prevalence of sick sinus syndrome is approximately 1 in 600 individuals older than 65 years - Can occur as tachy-brady syndrome/brady-tachy syndrom • Sick sinus syndrome leading to sinus bradycardia may be caused by degenerative changes in the sinus node that occur with advancing age 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 34
- 35. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 35
- 36. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 36
- 37. Treatment • Treatment of sinus bradycardia is only necessary in patients who become symptomatic • The patient is taking any medication(s) that may cause symptomatic sinus bradycardia, they should be discontinued whenever possible • Acute hemodynamically unstable patient: atropine • Hemodynamically unstable with severe symptoms unresponsive to atropine: adrenaline and/or dopamine • Long-term management of patients with sick sinus syndrome requires implantation of a permanent pacemaker 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 37
- 38. AV Nodal Block • AV nodal block occurs when conduction of electrical impulses through the AV node is impaired to varying degrees • Classified as 1. First degree 2. Second degree (Mobitz type I (also known as Wenckebach) and Mobitz type II) 3. Third degree heart block ( complete heart block) 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 38
- 39. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 39
- 40. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 40
- 41. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 41
- 42. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 42
- 43. Treatment • Similar to treatment of symptomatic sick sinus syndrome 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 43
- 44. Atrial Fibrillation • Arrythmias that need clinician attention. Why? - AF is the most common arrhythmia encountered in clinical practice - It is important for clinicians to understand AF because it is associated with substantial morbidity and mortality - Some drugs used to treat AF have a narrow therapeutic index and a broad adverse effect profile 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 44
- 45. AF: epidemiology and Etiology • The prevalence of AF increases with advancing age; roughly 8% of patients between the ages of 80 and 89 years have AF • Common in men than women • Hypertension, CAD, HF is increasingly recognized as a cause of AF - HF is increasingly recognized as a cause of AF; approximately 25% to 30% of patients with New York Heart Association (NYHA) class III HF have AF and the arrhythmia is present in as many as 50% of patients with NYHA class IV HF • Drug-induced AF is relatively uncommon 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 45
- 46. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 46
- 47. Pathophysiology • AF may be caused by both abnormal impulse formation and abnormal impulse conduction • AF is triggered by electrical impulses generated within the pulmonary veins • A substantial amount of the atrial electrical activity occurring during AF is conducted through the AV node into the ventricles, resulting in ventricular rates ranging from 100 to 200 beats/min • Classified in to paroxysmal, persistent an permanent 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 47
- 48. Complications of AF • AF is associated with substantial morbidity and mortality - The risk of stroke is increased two to sevenfold in patients with AF compared to patients without this arrhythmia - Patients with AF are also at increased risk for systemic thromboembolism - AF is associated with a threefold increase in the risk of HF as a result of tachycardia-induced cardiomyopathy - AF increases the risk of dementia and mortality approximately twofold compared to patients without AF 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 48
- 49. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 49
- 50. Treatment • The goals of individualized therapy for AF are: (a) ventricular rate control (b) termination of AF and restoration of sinus rhythm (commonly referred to as “cardioversion” or “conversion to sinus rhythm”) (c) maintenance of sinus rhythm, or reduction in the frequency of episodes of paroxysmal AF and/or (d) prevention of stroke and systemic thromboembolism 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 50
- 51. Treatment Goals According to AF Classification 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 51 Ventricular Rate Control Ventricular rate control can be achieved by inhibiting the proportion of electrical impulses conducted from the atria to the ventricles through the AV node
- 52. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 52
- 53. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 53
- 54. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 54
- 55. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 55
- 56. Conversion to Sinus Rhythm • Termination of AF in hemodynamically stable patients may be performed using antiarrhythmic drug therapy or elective DCC • DCC is generally more effective than drug therapy for conversion of AF to sinus rhythm 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 56
- 57. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 57
- 58. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 58
- 59. Maintenance of Sinus Rhythm/Reduction in the Frequency of Episodes of Paroxysmal AF • amore realistic goal for many patients is not permanent maintenance of sinus rhythm, but rather reduction in the frequency of episodes of paroxysmal AF • Maintenance of sinus rhythm is more likely to be successful in patients with AF duration of less than 6 months • Studies are available to compare maintenance of sinus rhythms versus rate control - No significant difference in terms of mortality - Increased hospitalization and adverse drug effects • Therefore, drug therapy for the purpose of maintaining sinus rhythm or reducing the frequency of episodes of AF should be initiated only in those patients with episodes of paroxysmal AF who continue to experience symptoms despite maximum tolerated doses of drugs for ventricular rate control 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 59
- 60. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 60
- 61. Prevention of Stroke and Systemic Thromboembolism • Most patients with paroxysmal, persistent, or permanent AF should receive therapy for prevention of thromboembolism unless compelling contraindications exist • In general, most patients require oral anticoagulation; however, in patients with nonvalvular AF and a CHA2DS2-VASc score of 0, anticoagulation is not recommended 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 61
- 62. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 62
- 63. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 63
- 64. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 64
- 65. Ventricular tachy arrythymia life-threatening ventricular tachyarrhythmias (Sustained ventricular tachycardia and ventricular fibrillation) torsades de pointes normal heart ventricular tachycardia non-sustained ventricular tachycardia ventricular premature beats 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 65
- 66. Ventricular Arrhythmias Ventricular tachycardia (VT) A condition in which an electrical signal is sent from the ventricles at a very fast but often regular rate. The ECG shows a rapid ventricular rhythm with broad (often 0.14 s or more), abnormal QRS complexes. AV dissociation may result in visible P waves Treatment: in haemodynamically compromised patients, emergency DC cardioversion may be required. If the blood pressure and cardiac output are well maintained, intravenous therapy with class I drugs or amiodarone is usually used. First-line drug treatment consists of lidocaine (50-100 mg i.v. over 5 minutes) followed by a lidocaine infusion (2-4 mg i.v. per minute). DC cardioversion is necessary if medical therapy is unsuccessful. 66 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa
- 67. Ventricular Tachycardia 67 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa
- 68. Ventricular Arrhythmias Ventricular fibrillation (VF) A condition in which many electrical signals are sent from the ventricles at a very fast and erratic rate. As a result, the ventricles are unable to fill with blood and pump. This rhythm is life-threatening because there is no pulse and complete loss of consciousness. The ECG shows shapeless, rapid oscillations and there is no hint of organized complexes A person in VF requires prompt defibrillation to restore the normal rhythm and function of the heart. It may cause sudden cardiac death. Basic and advanced cardiac life support is needed Survivors of these ventricular tachyarrhythmias are, in the absence of an identifiable reversible cause (e.g. acute myocardial infarction, severe metabolic disturbance), at high risk of sudden death. Implantable cardioverter-defibrillators (ICDs) are first-line therapy in the management of these patients 68 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa
- 69. Ventricular Fibrillation 69 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa
- 70. 70 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa
- 71. 71 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa
- 72. 72 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa
- 73. Torsades de Pointes • Torsades de Pointes (TdP) is a specific polymorphic VT associated with prolongation of the QT interval in the sinus beats that precede the arrhythmia 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 73
- 74. Etiology and pathophysiology • Inherited or acquired • TdP is caused by circumstances, often drugs, that lead to prolongation in the repolarization phase of the ventricular action potential • Prolongation of ventricular repolarization promotes the development of early ventricular afterdepolarizations during the relative refractory period, which may provoke reentry leading to TdP • Drug-induced TdP rarely occurs in patients without specific risk factors for the arrhythmia 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 74
- 75. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 75
- 76. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 76
- 77. Treatment • Desired outcomes include (a) prevention of TdP, (b) termination of TdP, (c) prevention of recurrence, and (d) prevention of sudden cardiac death 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 77
- 78. Treatment • Hemodynamically stable TdP is often treated with IV magnesium sulfate, irrespective of whether the patient is hypomagnesemic; magnesium has been shown to terminate TdP in normomagnesemic patients • Magnesium sulfate should be administered IV in doses of 1 to 2 g, diluted in 50 to 100 mL 5% dextrose in water (D5W), administered over 5 to 10 minutes; doses may be repeated to a total of 12 g • Alternatively, a continuous magnesium infusion (0.5 to 1 g/hour) may be initiated after the first bolus 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 78
- 79. 9/23/2021 Arrythmia for 4th year regular by Tolcha Regasa 79