Necrotising soft tissue infection.pptx
•Download as PPTX, PDF•
0 likes•7 views

Necrotising soft tissue infection- etiologies and management

Recommended
More Related Content
Similar to Necrotising soft tissue infection.pptx
Similar to Necrotising soft tissue infection.pptx (20)
Recently uploaded
Recently uploaded (20)
Necrotising soft tissue infection.pptx
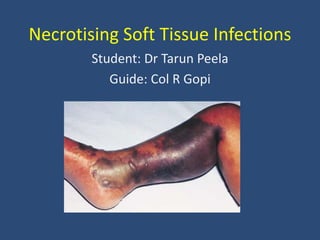
- 1. Necrotising Soft Tissue Infections Student: Dr Tarun Peela Guide: Col R Gopi
- 2. Introduction • Infection – – soft tissue compartment (dermis, subcutaneous tissue, superficial fascia, deep fascia, or muscle) – necrosis • Inocuous wound, rapid spread, sepsis • Surgery is the cure
- 3. History • Hippocrates - 5th century BC. • British surgeon Leonard Gillespie - late 18th century --as phagedaenic ulcer • Confederate Army surgeon Joseph Jones in 1871 from USA -- term hospital gangrene • Wilson- Necrotizing fasciitis- 1951 • Later NSTI
- 4. Etiology – Trauma – IV drug and insulin injection – skin infections and ulcers – animal and insect bites – surgical complications – percutaneous catheter insertion – Abscesses – idiopathic etiologies Inoculation of the pathogen into the subcutaneous tissue via any break in an epithelial or mucosal surface • More vulnerable • Diabetics • Obese • Immunocompromised • Peripheral vascular disease
- 5. Clinical features • Giuliano and colleagues 1977 - Classified • Three types basing on pathogen Type 1 Type 2 Type 3 Polymicrobial source • Gram-positive cocci • Gram-negative rods • Anaerobes (Bacteroides species, Clostridium perfringens and septicum) Monomicrobial infection • β-hemolytic streptococci or • staphylococci (MRSA rising in frequency to 40%) V. vulnificus infection
- 6. Type 1 Type 2 Type 3 • 55-75% • Elderly with comorbidities • 20-50% risk factor not identified • Clostridium perfringens, C. septicum, and C. sordellii • Symptomatic within hours • α-toxin • 15-25% • Healthy hosts • Associated with toxic shock • Streptococcal M proteins • Superantigen activity • 5% • Sea divers • oyster ingestion by chronic liver dis • Warm-water coastal regions • Apoptosis of lympho/neutro • Early evidence of significant systemic toxicity • Multisystem organ failure and cardiovascular collapse occur very early
- 7. Clinical features • Hallmark- Rapid progression of disease • Strong suspicion – An apparent superficial cellulitis progresses rapidlyfails to respond to standard therapy evolving systemic signs of sepsis
- 8. Clinical features Early features Late features • Pain out of proportion to examination • Erythema • Hyperthermia • Edema beyond the area of erythema • Skin anaesthesia • Epidermolysis • Bronzing of skin • Tachycardia • Fever • Hemorrhagic bullae • Foul odour • Brownish-tan “dishwater” drainage • Dermal gangrene • Crepitus • Severe pain out of proportion to exam • Sepsis • Shock • Organ failure
- 9. Evaluation • Chin-Ho Wong, Md et al The LRINEC score: A tool for distinguishing necrotizing fasciitis from other soft tissue infections Crit Care Med 2004 Vol. 32, No. 7
- 10. LRINEC score • Low risk- <5 • Mod risk- 6-7(positive predictive value 92.0%) • High risk- >8(positive predictive value 93.4%)
- 11. • Serum lactate>6 mmol/L alone- 32% mortality • Serum sodium level >-135 mEq/L with lactate <6mmol/L - 0% mortality • Arezou Yaghoubian, MD et al. Use of Admission Serum Lactate and Sodium Levels to Predict Mortality in Necrotizing Soft-Tissue Infections Arch Surg. 2007;142(9):840-846
- 12. • Procalcitonin ratio of POD1:POD2- • >1.14 - successful eradication of the infectious focus • Jan Friederichs, M.D. et al. Procalcitonin ratio as a predictor of successful surgicaltreatment of severe necrotizing soft tissue infections Am j surg 2013
- 13. Imaging • Delay caused by imaging outweighs its potential benefit • Plain film radiography- subcutaneous emphysema- specific finding for clostridial NSTI
- 14. Imaging • CT is more sensitive than plain radiography – fascial thickening – edema – subcutaneous gas – abscess formation • Magnetic resonance imaging sensitive but lacks specificity • Ultrasonography lacks sensitivity or specificity
- 15. Diagnosis • Strong history and physical examination • “finger test” – a 2-cm incision is made down to the deep fascia – gentle probing with the index finger – positive finger test – lack of bleeding, presence of characteristic “dishwater pus,” and lack of tissue resistance • High clinical suspicion- Exploration not delayed • Gold standard - operative
- 16. Management • Proper patient triage to an ICU • Resuscitation with IV fluids • Nutrition • Antibiotics • Surgery
- 17. Antibiotics G+ G- Anaerobes MRSA Penicillins Third-generation cephalosporin or aminoglycosides Flouroquinolones Metronidazole/ clindamycin Vancomycin/ Linezolid • Clindamycin has relatively broad activity – Decrease α- toxin production by clostridial species – Reduce superantigen M protein by streptococcal species – Suppress LPS–induced TNF-α production by monocytes
- 18. Operative • Incisions – – extend at least beyond the area of induration – parallel to neurovascular bundles – extending to and exposing the deep fascia • Induration - dermal lymphatics are blocked and postcapillary venules are thrombosed, which lead to tissue necrosis
- 19. Operative • Necrotic tissue - dull, gray, and avascular- excised • Characteristic “murky dishwater”– like fluid • Non contractile muscle • Thrombosed vessels • No resistance at fascial planes • Borders for debridement • Where tissue planes cease to readily separate • Healthy bleeding tissue at all margins
- 20. Operative • Aggressive debridement- en mass organs, tissues, and structures • Joint involvement- amputation • Rapid quantitative tissue cultures (if available) and frozen section analysis may help guide the debridement
- 21. Repeat debridements • Revision surgery (“second look”) within 24 to 48 hours • Progressive necrosis – – polymicrobial synergy – infectious spread – hypotension • Adjuncts to surgery include topical antimicrobial creams, subatmospheric pressure wound dressings, and optimization of nutrition.
- 22. Wound care • The goals of treatment – to achieve a clean wound – protect it from dessication – Assess the need for further surgical debridement – promote wound healing • Prevent exposed tendons, bone, or cartilage from dessication
- 23. Wound care • Wound dressings - promote mobility of the patient - prevent nosocomial complications such as pneumonia, UTI,DVT • Should not impede the range of motion of the joint or extremity • Should not pull the tissue into a position of deformity.
- 24. Wound coverage and reconstruction • Primary closure • Split-thickness skin grafts • Full-thickness skin grafts • Delayed primary closure vs healing by secondary intention • Tissue expansion • Pedicled or free flaps.
- 27. Skin sparing technique • Perfused skin beyond the margins of the frankly necrotic tissue should be preserved • Limits excision of viable overlying skin and subcutaneous tissue hence – a “skin-sparing” debridement. Laura K. Tom, MD et al. A Skin-Sparing Approach to the Treatment of Necrotizing Soft Tissue Infections: Thinking Reconstruction at Initial Debridement. Journal of the American College of Surgeons. Jan 2016
- 28. Skin sparing technique • Incision design – Over the most obviously infected, discolored or necrotic area – Place longitudinally on extremities – Avoid incisions perpendicular to flexion creases – Avoid incisions directly over boney prominences, large vessels and nerves
- 29. Skin sparing technique • Exposure and Troubleshooting – Elevate full thickness skin and subcutaneous flaps – Lengthen linear longitudinal incisions – Use trap door or counter incisions • Debridement – Excise ALL necrotic tissue – leave viable tissue – Debride overlying skin if it is necrotic – Plan for repeat examinations under anesthesia
- 31. HBOT • Delivery of oxygen at 2-3 times typical atmospheric pressure • Leads to arterial oxygen tension as high as 2000 mm Hg with resulting tissue oxygen tension of 300 mm Hg(arterial oxygen tension of 300 mm Hg and tissue oxygen tension of 75 mm Hg ) • Elevated levels of oxygen at the tissue level – reduce edema – stimulate fibroblast growth – increase the killing ability of leukocytes by augmenting the oxidative burst – independent cytotoxic effects on some anaerobes • No differences in mortality or length of stay *George ME, Rueth NM, Skarda DE, et al: Hyperbaric oxygen does not improve outcome in patients with necrotizing soft tissue infection. Surg Infect (Larchmt) 2009; 10:21–28
- 32. IVIG • Pooled IVIg from human donors • Binds exotoxins produced by staphylococcal and streptococcal bacterial infections • Limits systemic inflammatory response • Limited to critically ill patients with only staphylococcal or streptococcal NSTIs or both • Hypersensitivity reactions
- 33. Rehabilitation • The aims – minimize the adverse effects caused by the injury in terms of healing the wound – minimizing the development and effect of scarring – maximizing functional outcomes – providing support to maximize psychological well- being and reintegration into society • Physical, psychological, and social aspects of care for the patient
- 34. References • Schwartz Principles of Surgery 10th e • Timo W. Hakkarainen et al. Necrotizing soft tissue infections: Review and current concepts in treatment, systems of care, and outcomes. Curr Probl Surg. 2014 August 51(8): 344–362. • Laura K. Tom, MD et al. A Skin-Sparing Approach to the Treatment of Necrotizing Soft Tissue Infections: Thinking Reconstruction at Initial Debridement. Journal of the American College of Surgeons. Jan 2016 • Ho H. Phan et al Necrotizing soft tissue infections in the intensive care unit Crit Care Med 2010 Vol. 38, No. 9 (Suppl.)
Editor's Notes
- Wong et al