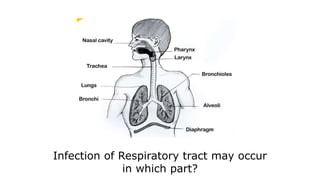
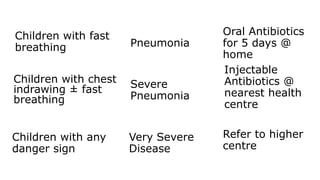
Acute respiratory infections can start in any part of the respiratory tract from the nose to the alveoli. In 1980, the WHO developed a pneumonia control strategy that uses simple signs to classify pneumonia severity and recommend appropriate treatment - oral antibiotics at home for non-severe cases and injectable antibiotics at a health center for severe cases. After 30 years, the WHO revised their pneumonia treatment guidelines to change the first-line antibiotic recommendation, redefine severity classifications, and recommend 3 days of oral amoxicillin for non-severe cases and parenteral ampicillin and gentamicin as first-line treatment for severe pneumonia cases.