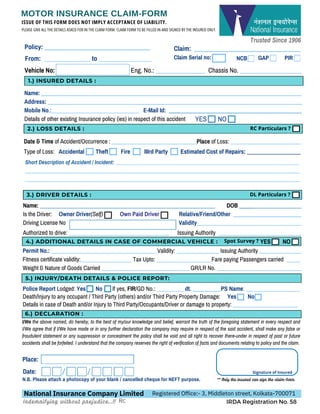
Vehicle No: Eng.No.: ________________ Chassis No. ____________________
1)
Name: ____________________________________________________________________________________________
Address: __________________________________________________________________________________________
Mobile No.:_______________________________ E-Mail Id: _______________________________________________
Details of other existing Insurance policy (ies) in respect of this accident NO
YES
I/We the above named, do hereby, to the best of my/our knowledge and belief, warrant the truth of the foregoing statement in every respect and
I/We agree that if I/We have made or in any further declaration the company may require in respect of the said accident, shall make any false or
fraudulent statement or any suppression or concealment the policy shall be void and all right to recover there-under in respect of past or future
accidents shall be forfeited. I understand that the company reserves the right of verification of facts and documents relating to policy and the claim.
Date & Time of Accident/Occurrence : ______________________________Place of Loss: _________________________
Type of Loss: Accidental Theft Fire IIIrd Party Estimated Cost of Repairs: ___________________
Name: ______________________________________________________________ DOB ______________________
Is the Driver: Owner Driver(Self) Own Paid Driver Relative/Friend/Other ________________________
Driving License No Validity_____________________________________
1.) INSURED DETAILS :
2.) LOSS DETAILS :
MOTOR INSURANCE CLAIM-FORM
ISSUE OF THIS FORM DOES NOT IMPLY ACCEPTANCE OF LIABILITY.
PLEASE GIVE ALL THE DETAILS ASKED FOR IN THE CLAIM FORM. CLAIM FORM TO BE FILLED IN AND SIGNED BY THE INSURED ONLY.
N.B. Please attach a photocopy of your blank / cancelled cheque for NEFT purpose.
National Insurance Company Limited Registered Office:- 3, Middleton street, Kolkata-700071
IRDA Registration No. 58
Indemnifying without prejudice...!!
Place:
Date: Signature of Insured
** Only the insured can sign the claim-form.
Short Description of Accident / Incident: _______________________________________________________________________
_________________________________________________________________________________________________
_________________________________________________________________________________________________
3.) DRIVER DETAILS :
Authorized to drive: ___________________________________ Issuing Authority _____________________________
4.) ADDITIONAL DETAILS IN CASE OF COMMERCIAL VEHICLE :
Permit No.: _____________________________________ Validity: _______________ Issuing Authority _______________
Fitness certificate validity:__________________ Tax Upto: ___________________ Fare paying Passengers carried _____
Weight & Nature of Goods Carried _______________________________ GR/LR No. ______________________________
5.) INJURY/DEATH DETAILS & POLICE REPORT:
6.) DECLARATION :
Trusted Since 1906
RC Particulars ?
DL Particulars ?
Police Report Lodged: Yes No If yes, FIR/GD No.: __________dt. __________PS Name: ___________________
Death/Injury to any occupant / Third Party (others) and/or Third Party Property Damage: Yes No
Details in case of Death and/or Injury to Third Party/Occupants/Driver or damage to property: _______________________
NO
YES
Spot Survey ?
Claim: ___________________________
_______
Policy: __________________________________
From: _______________ to _________________ NCB GAP PIR
Claim Serial no:
Rc
2.
Trusted Since 1906
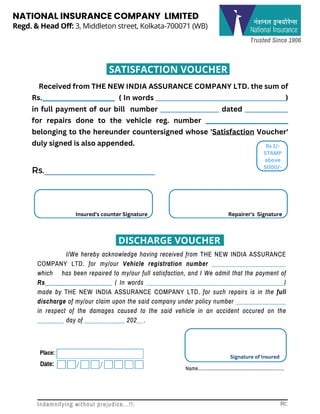
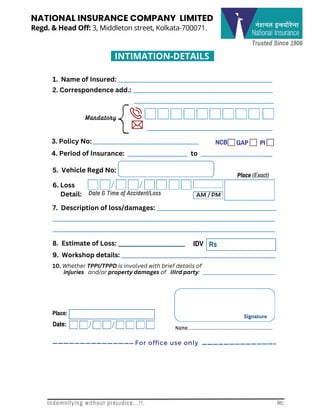
Regd.& Head Off: 3, Middleton street, Kolkata-700071 (WB)
NATIONAL INSURANCE COMPANY LIMITED
SATISFACTION VOUCHER
Received from THE NEW INDIA ASSURANCE COMPANY LTD. the sum of
Rs.______________________ ( In words __________________________________________)
in full payment of our bill number ___________________ dated ______________
for repairs done to the vehicle reg. number _________________________
belonging to the hereunder countersigned whose 'Satisfaction Voucher'
duly signed is also appended.
I/We hereby acknowledge having received from THE NEW INDIA ASSURANCE
COMPANY LTD. for my/our Vehicle registration number ______________________
which has been repaired to my/our full satisfaction, and I We admit that the payment of
Rs____________________ ( In words _________________________________________)
made by THE NEW INDIA ASSURANCE COMPANY LTD. for such repairs is in the full
discharge of my/our claim upon the said company under policy number _______________
in respect of the damages caused to the said vehicle in an accident occured on the
________ day of ____________ 202__.
Place:
Date:
Signature of Insured
Name..............................................................
Rs
Rs 1/-
STAMP
above
5000/-
Rs.______________________
Insured's counter Signature Repairer's Signature
Indemnifying without prejudice...!!. Rc
DISCHARGE VOUCHER
3.
Trusted Since 1906
Regd.& Head Off: 3, Middleton street, Kolkata-700071.
NATIONAL INSURANCE COMPANY LIMITED
INTIMATION-DETAILS
Date & Time of Accident/Loss AM / PM
NCB GAP PI
IDV
6. Loss
Detail:
1. Name of Insured: ______________________________________________________
2. Correspondence add.: _________________________________________________
__
_______________________________________________
______________________________________
3. Policy No: _____________________________________
4. Period of Insurance: _____________________ to _________________________
5. Vehicle Regd No:
Place (Exact)
7. Description of loss/damages: __________________________________________
______________________________________________________________________________
______________________________________________________________________________
8. Estimate of Loss: ______________________
10. Whether TPPI/TPPD is involved with brief details of
injuries and/or property damages of IIIrd party: ______________________________
9. Workshop details: ______________________________________________________
Rs
Place:
Date:
Signature
Name..............................................................
Mandatory
For office use only
Indemnifying without prejudice...!!. Rc