
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Hydrocephalus
Similar to Hydrocephalus (20)
Recently uploaded
Recently uploaded (20)
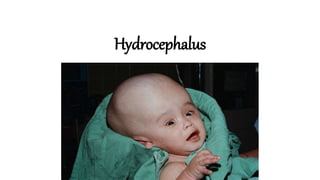
Hydrocephalus
- 2. •It is an excessive accumulation of CSF in the ventricles and subarachnoid space of the brain. • Hydrocephalus is commonly called “water on the brain.” •It is a combination of the Greek word “hydro,” ---water and “cephalus” --- head.
- 3. What is CSF? • CSF looks like water, but it contains proteins, electrolytes, and nutrients that help to keep brain healthy. • The most important purpose of CSF is to cushion brain and spinal cord against injury. • Brain produces 20 ml of CSF per hour and 3-4 lit per day. • It circulates through a network of tiny passageways in brain, and ultimately into blood stream where it is absorbed by body.
- 4. Overview of CSF production • The choroid plexuses are the source of approximately 80% of the CSF • The blood vessels in the subependymal regions, and pia also contribute to the formation of CSF
- 5. CSF circulation Choroid plexus of lateral ventricles Foramen Monro Third ventricle Aqueduct of sylvie Fourth Ventricle Foramen of Magendie and Luschka Subarachinoid space
- 6. CSF pressure • Normal intracranial pressure (ICP) in an adult is between 2-8 mmHg. • Levels up to 16 mmHg are considered normal • ICP higher than 40 mmHg or lower BP may combine to cause ischemic damage
- 7. ETIOLOGY • 1. Over production of CSF by choroid plexus --- Tumor --- Inflammation • 2. Obstruction in the passage of CSF --- Congenital atresia / narrow aqueduct of sylvius --- Infections – meningitis, encephalitis --- Tumor / haemorrhage / adhesion • 3. Inadequate absorption of CSF --- In extensive subarachinoid haemorrhage
- 8. CLASSIFICATIONS I. a. Communicating / Non- Obstructive Hydrocephalus No blockage between ventricular system,basal cisterns & spinal arachinoid space. It is due to --- failure in absorption of CSF. eg. Cavernous sinus thrombosis --- over production of CSF. eg. choroid plexus papilloma, pseudotumor of cerebri b. Non- Communitcating / Obstructive Hydrocephalus Blockage at any level of CSF pathway It is due to --- obstructive lesion / inflammation Obstruction ------- partial ------- intermittent ------- complete
- 9. • II. A. Congenital Hydrocephalus Causes: Intrauterine infection ( TORCH ) Congenital malformation – aqueduct stenosis Dandy walker syndrome – Congenital septa /membrane block the forth ventricle outlet Arnold – chiari malformation – displacement of the brain stem and cerebellum into upper cervical part of spine through foramen magnum
- 10. • b. Acquired Hydrocephalus Causes Inflammatory meningitis / encephalitis Traumatic birth injury / head injury/ ICH ICSOL- tuberculoma, abscess,glioma Connective tissue disorder
- 11. PATHOPHYSIOLOGY Non- communitating hydrocephalus communitating hydrocephalus Blockage in between the ventricular & increased production / poor Subarachnoid space absorption of CSF Interference with the CSF circulation
- 12. Dilation of ventricles & compression of brain tissue Enlargement of skull Increased ICP
- 13. CLINICAL MANIFESTATIONS Newborns & Infants oLarge skull with separated sutures oAnt fontanel – intense & bulged oThinning of skull bones oMacewen sign – cracked pot sound on percussion Infants ( later) – ounequal response to light oSun setting eyes – visible sclera above iris oFrontal bossing, sluggish pupils, depressed eye Infants ( in general ) • Irritability, shrill ,high pitch cry • Lethargy, opisthotonos • Persistent early infantile reflexes • Change in LOC • Vomiting • Lower extremity spasticity • Difficulty in sucking & feeding
- 14. Older children Headache on awakening Papilledema Strabismus Ataxia Irritability Lethargy Confusion Apathy Incontinence Vomiting Signs of increased ICP & meningeal irritation Sun setting sign
- 15. DIAGNOSIS • History collection & physical examination • EEG • CT & MRI • X- ray • Pneumoencephalography • Ophthalmoscopy • CSF analysis
- 16. MANAGEMENT Pharmacological management Acetazolamide – 50 mg/kg/day ( to decrease CSF production ) Oral glycerol & isosorbide Antibiotics Surgical management Removal of obstruction in CSF flow Ventriculostomy- destruction of portion of choroid plexus Shunting of CSF from ventricle to another normal site in CSF pathway Shunting of CSF from ventricle to an area outside CNS system
- 17. Types of extra cranial shunts 1. Ventriculoperitoneal shunt – Common Through a burr hole in the skull ventricular catheter is inserted into ant. Portion of lateral ventricle. A valve unit is tested & attached to the catheter. An incision is made in the abdomen & through the rectus muscle in to the peritoneum. Here CSF is absorbed by tissues in the abdominal cavity
- 18. 2. Ventriculoatrial shunt Catheter from lateral ventricle to RA of heart Here CSF drains into circulating blood. 3. Ventriculoureter shunt Here CSF drains through ureter & into the urinary bladder Used in older children / if other two methods fails. 4. Ventriculopleural shunt Here CSF drains into the pleural cavity.
- 19. NURSING MANAGEMENT Preoperative Assess for any signs of increased ICP Monitor head circumference Assess vital signs frequently Assess for any signs of dehydration Postoperative Assess vital signs every 15 – 30 mints & monitor I/O chart. Administer oxygen Position-bed head elevation 15- 300 Assess for any signs of increased ICP Assess for LOC & pupillary reactions Assess patency of the shunt Assess the nutritional status of the child Assess for any complications
- 20. • Than you