Download as PDF, PPTX

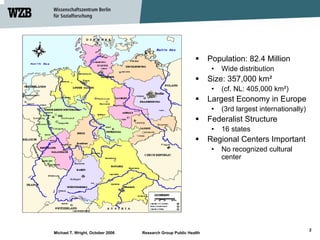


The document discusses the political context of community-based prevention research in Germany, highlighting its federal structure and emphasis on health as a state responsibility. It examines the current health insurance model, prevention laws, and strategies to address health inequalities, particularly through community engagement. The author advocates for the recognition of political factors in community-based research and the development of local knowledge into evidence to effect social change.



































































