
Recommended
More Related Content
What's hot
What's hot (20)
Similar to TYPES OF OESOPHAGEAL ATRESIA.pptx
Similar to TYPES OF OESOPHAGEAL ATRESIA.pptx (20)
Recently uploaded
Recently uploaded (20)
TYPES OF OESOPHAGEAL ATRESIA.pptx
- 1. TYPES OF OESOPHAGEAL ATRESIA SUBMITTED BY: SMRUTI REKHA DAS ROLL NO: 2188012 MSc NURSING 1st YEAR
- 2. What is oesophageal atresia ? • Oesophageal atresia is a birth defect in which part of a baby's oesophagus does not develop properly. • Oesophageal atresia is a birth defect of the swallowing tube (oesophagus) that connects the mouth to the stomach.
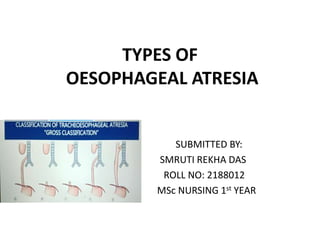
- 3. Types of Oesophageal Atresia Vogt classified Oesophageal Atresia into 5types. Those are • Types I • Types II • Types III • Types IV • Types V
- 5. Oesophageal Atresia type I • In this type, there is oesophageal atresia and proximal and distal segments of oesophagus are blind. There is no communication between trachea and oesophagus. • This type is presrent in 3-7% of cases.
- 6. Oesophageal Atresia type II • In this type, oesophageal atresia is present and the blind proximal segment of oesophagus connects with trachea by a fistula.The distal end of oesophagus is blind. • This type is present in 0.8% cases.
- 7. Oesophageal Atresia type III • In this type, oesophageal atresia is present.The proximal end of oesophagus is a blind pouch and distal segment of oesophagus is connected by fistula to trachea. • This is the commonest type,present in 87% cases.
- 8. Oesophageal Atresia IV • In this type, both upper and lower segments of oesophagus communicate with trachea. • It is the rearest type that occures in 0.7% cases.
- 9. Oesophageal Atresia Type V • In this type, oesophagus and trachea are normal and completely formed but are connected by a fistula. • This type is known as ‘H’ type and is presented in 4.2% cases.
- 10. Treatment Once a diagnosis has been made, surgery is needed to reconnect the two ends of the esophagus so that the baby can breathe and feed properly. Multiple surgeries and other procedures or medications may be needed, particularly if the baby’s repaired esophagus becomes too narrow for food to pass through it; if the muscles of the esophagus don’t work well enough to move food into the stomach; or if digested food in the stomach consistently moves back up into the esophagus.
- 11. Nursing Intervention • A nasogastric tube is put in the upper oesophageal segment and is aspirated frequently, to prevent collection and aspiration of secretion into the trachea. Intravenous fluids are administered to maintain the hydration status of infant. Place the infant in semi- upright position and administer oxygen if cyanosis is present. • A cervical oesophagostomy is made to drain out secretions from blind oesophageal pouch and administer oxygen to infant. Feed the infant orally or by gastrostomy. Position the baby comfortably in semi- fowler’s position and administer analgesics.
- 12. Conclusion Without a working oesophagus, it's impossible to receive enough nutrition by mouth. Babies with oesophagus atresiaare also more prone to infections like pneumonia and conditions such as acid reflux. Luckily, oesophagus atresia is usually treatable.
- 13. Bibliography • Sharma Rimple,Essentials of Pesiatric nursing,JAYPEE Brothers medical publishers(P),Page no 351-355. • www.wikipedia.com • www.slideshare.com
- 14. THANK YOU