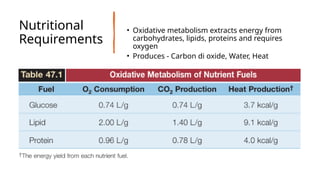
• Combined metabolismof all nutrients determines:
• Oxygen consumption (VO₂)
• Carbon dioxide production (VCO₂)
• Heat production
• 24-hour heat production = Daily Energy Expenditure (DEE) -
DEE guides caloric prescription in nutritional support
• Based on the principal of indirect calorimetry , Resting Energy
Expenditure (REE) is calculated.
• REE (kcal/min) = (3.6 × VO₂) + (1.1 × VCO₂) – 61
• DEE = REE (kcal/min) x 1440 Minutes (kcal/ day)
• Simple Predictive Formula (recomended routinely and
ACCURATE in ICU pt)
• REE (kcal/day) = 25 × body weight (kg)
4.
• Actual bodyweight is used as long as patient is not obese
• If actual body wt is 25% higher than ideal body weight –
adjusted body weight used.
• Adjusted wt (kg) = [(Actual – Ideal) × 0.25] + Ideal wt
5.
• Daily energyneeds are met by non-protein calories:
Carbohydrates, Lipids
• Protein is reserved for: Enzymatic functions, Structural protein
maintenance
• Carbohydrates - Provide ~70% of nonprotein calories and have
limited body stores daily intake essential
→
• Critical for : CNS Function
• Excess : Hyperglycemia ,Impaired immune function
• Lipids - ~30% of daily energy with Highest energy yield
• Adipose tissue is the main endogenous fuel reserve in healthy adults
Nutritional Requirements – Substrate
6.
• Propofol –formulated in 10% Lipid emulsion and provides 1.1
kcal/ml ; Calories must be included in non-protein calorie
calculations
Protein Requirements
• Normal intake: 0.8–1 g/kg/day
• ICU patients: 1.2–1.6 g/kg/day - Increased needs due to:
Hypercatabolic state
• Nitrogen Balance - Assesses adequacy of protein intake ;
Defined as- (Nitrogen intake – nitrogen excretion)
• Nitrogen Excretion - ~⅔ excreted in urine ; ~85% as urea measured
as Urinary Urea Nitrogen (UUN)
• Non-urinary losses: ~4–6 g/day (stool but unreliable in diarrhea)
• Nitrogen Excretion (g/day)= UUN + (4–6)
7.
• Nitrogen Intake
•Protein is 16% nitrogen
• 1g Protein contains 1/6.25 g of Nitrogen
• Nitrogen Intake (g/day) = Protein intake (g/day) / 6.25
• Nitrogen Balance (g/day) - (Protein / 6.25) – [UUN + (4–6)]
GOAL OF NUTRION -positive nitrogen balance of 4–6 grams.
8.
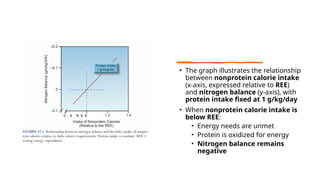
• The graphillustrates the relationship
between nonprotein calorie intake
(x-axis, expressed relative to REE)
and nitrogen balance (y-axis), with
protein intake fixed at 1 g/kg/day
• When nonprotein calorie intake is
below REE:
• Energy needs are unmet
• Protein is oxidized for energy
• Nitrogen balance remains
negative
9.
• At nonproteincalorie intake REE
≈ :
• Energy requirements are just met
• Nitrogen balance approaches zero
• When nonprotein calories exceed REE:
• Adequate energy is available from carbohydrates and lipids
• Protein is spared from oxidation
• Nitrogen balance becomes positive
• TAKE HOME MESSAGE –
• Adequate nonprotein calories are essential to achieve a positive nitrogen balance
• Increasing protein intake alone is ineffective unless energy needs (REE) are met or
exceeded
• This figure visually reinforces the concept of protein sparing by nonprotein calories
10.
Ideal Body Weightand Basal Energy Expenditure (BEE)
IDEAL BODY WT (DEVINE FORMULA) :
• Males = 50 kg + 0.9 kg × (height (cm) 152)
−
• Female = 45.5 kg + 0.9 kg × (height (cm) 152)
−
BASAL ENERGY EXPENDITURE: It is amount of energy required to
maintain the body’s basic metabolic functions while at rest.
BEE calculation (Harris-Benedict equation):
• Men: 66 + (13.7 x W) + (5 x H) – (6.8 x A)
• Women: 65.5 + (9.6 x W) + (1.8 x H) – (4.7 x A)
W = Weight in Kg, H = Height in centimetres, A = Age in years
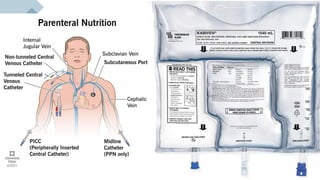
PARENTRAL NUTRITION
• Malnutritionassociated by starvation is due to abnormal
nutrient processing and not due to starvation.
• Metabolic changes in critical illness
• Protein catabolism
• BMR increases by up to 40%
• State of relative insulin resistance
• Infusion of nutrient solutions into the blood stream via a
peripheral vein/central venous access
• Gut should be the preferred route (Oral >>
Enteral>Parentral)
SUBSTRATE SOLUTIONS
A. DEXTROSESOLUTION
• Dextrose (glucose) is the
carbohydrate source for TPN
• Energy yield of dextrose is low,
requires highly concentrated
solutions
• Standard solution: 50% dextrose
(D50)
• Dextrose solutions are
hyperosmolar - Must be infused
via large central veins
17.
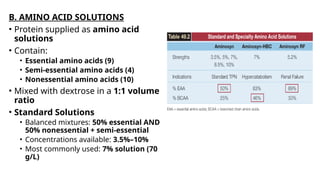
B. AMINO ACIDSOLUTIONS
• Protein supplied as amino acid
solutions
• Contain:
• Essential amino acids (9)
• Semi-essential amino acids (4)
• Nonessential amino acids (10)
• Mixed with dextrose in a 1:1 volume
ratio
• Standard Solutions
• Balanced mixtures: 50% essential AND
50% nonessential + semi-essential
• Concentrations available: 3.5%–10%
• Most commonly used: 7% solution (70
g/L)
18.
Specialty Solutions
• Designedfor: Severe metabolic stress , Renal failure, Hepatic failure
• Metabolic Stress Solutions - Enriched with branched-chain amino
acids (BCAA): Preferred skeletal muscle fuels during high metabolic
demand.
• Isoleucine
• Leucine
• Valine
• Renal Failure Solutions - Rich in essential amino acids ; Nitrogen
recycling reduces rise in blood urea nitrogen (BUN)
• Hepatic Failure Solutions - Enriched with BCAA ; Reduce transport of
aromatic amino acids across the BBB ; May reduce hepatic
encephalopathy
• Important: No specialty amino acid solution has shown improved
clinical outcomes
19.
Glutamine
• Primary fuelfor:
• Intestinal epithelial cells
• Vascular endothelial cells
• Shown to:
• Preserve bowel mucosal integrity
• Reduce infections in ICU patients
• Previously recommended dose: 0.2–0.4 g/kg/day
• Recent multicenter study: Increased mortality in ICU
patients with multiorgan failure
• Current status: Routine supplementation requires re-
evaluation
• Not included in commercial amino acid solutions
20.
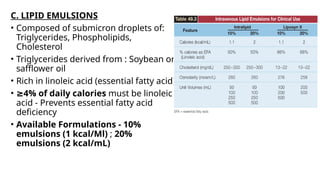
C. LIPID EMULSIONS
•Composed of submicron droplets of:
Triglycerides, Phospholipids,
Cholesterol
• Triglycerides derived from : Soybean or
safflower oil
• Rich in linoleic acid (essential fatty acid)
• ≥4% of daily calories must be linoleic
acid - Prevents essential fatty acid
deficiency
• Available Formulations - 10%
emulsions (1 kcal/Ml) ; 20%
emulsions (2 kcal/mL)
21.
ADDITIVES
• Commercial mixturesof: Electrolytes, Vitamins, Trace
elements; Added directly to dextrose–amino acid
mixtures
• Electrolytes - 15 commercially available electrolyte mixtures
• Typical volume: 20 mL
• Common contents: Sodium, Chloride, Potassium, Magnesium
• Composition varies by product - Check local hospital formulation
• Additional electrolyte needs (e.g., potassium): Must be specified in
TPN orders
22.
Vitamins
• Aqueous multivitaminpreparations added to TPN
• One standard vial provides: Normal daily requirements for most
vitamins
• ICU considerations: Actual requirements unknown
• Vitamin deficiencies common despite standard supplementation
• Suggests increased vitamin needs in critically ill patients
Trace Elements
• Multiple commercial trace element preparations available
• Poor correlation between: Recommended daily requirements and
content of commercial mixtures
• Trace element mixtures:
• Do not contain iron or iodine
• Some lack selenium
23.
Creating a TPNRegimen
Step wise approach, let us take an example of a 70kg, non-
malnourished patient with no volume restriction.
• STEP 1: DETERMINE DAILY CALORIE AND PROTEIN
REQUIREMENTS
oCalories: 25 kcal/kg/day (25 X 70 = 1,750 kcal/day)
oProtein: 1.2–1.6 g/kg/day (1.4 x 70 = 98g/day)
• Use actual body weight if 125% of ideal
≤
• Use adjusted body weight if >125% of ideal
• Indirect calorimetry preferred if available
oPropofol adjustment , 10% lipid emulsion provides 1 kcal/ml ;
subtract this from daily caloric requirement
26.
STEP 2: DETERMINEVOLUME OF DEXTROSE–AMINO ACID
MIXTURE
• Standard mixture: 10% amino acids (500 mL)-50%
dextrose (500 mL) (A10-D50)
• Final concentration: 5% amino acids (50 g protein/L) AND
25% dextrose (250 g/L)
• Required volume to meet protein needs: daily protein
requirement is equivalent to the daily protein requirement
(98 g/day), divided by the protein concentration in the amino
acid mixture (50 g/L
• Infusion rate over 24 hours:
• 1,900 mL ÷ 24 = ~80 mL/hr
27.
STEP 3: CALCULATEDEXTROSE CALORIES
• Dextrose content: 250 g/L × 1.9 L = 475 g
• Energy yield: 3.4 kcal/g
• Calories provided: 475 × 3.4 = 1,615 kcal/day
STEP 4: ADD LIPIDS TO MEET CALORIC DEFICIT
• Daily calorie requirement: 1,750 kcal
• Dextrose calories provided: 1,615 kcal
• Caloric deficit: 135 kcal
• Lipid source: 10% lipid emulsion (1 kcal/mL)
• Required volume: 135 mL/day (Adjust to 150 mL - available unit
volume)
• Maximum infusion rate: 50 mL/hr
28.
STEP 5: WRITETPN ORDERS (Example):
• A10–D50 at 80 mL/hr
• 10% Intralipid, 150 mL, over 3 hours
• Add standard electrolytes, multivitamins, and trace
elements
• TPN orders are rewritten daily
• Electrolytes, vitamins, and trace elements adjusted as
required
30.
COMPLICATIONS
Catheter-Related Complications
• Hyperosmolardextrose–amino acid solutions require:
Central venous catheter or Peripherally inserted central
catheter (PICC)
Misdirected Catheter
• Subclavian lines and PICCs may be misdirected into the
internal jugular vein
• Reported incidence: ~10% of subclavian vein cannulations
(mostly right-sided)
31.
Metabolic Complications
Hypophosphatemia
• Glucoseentry into cells causes intracellular phosphate shift
and phosphate utilization for metabolic cofactors
• Most common cause of hypophosphatemia in hospitalized
patients
• Plasma phosphate levels decline progressively after starting
TPN
32.
Hypokalemia
• Glucose uptakecauses intracellular potassium shift
• Effect usually transient
• Persistent hypokalemia may occur with continued glucose
loading during TPN
Hypercapnia
• Seen in patients with respiratory insufficiency
• Previously attributed to high respiratory quotient of
carbohydrates
• Actual cause: Overfeeding, not carbohydrate excess
33.
Lipid Complications
• Overfeedingwith lipids may cause: Hepatic steatosis
• Major concern: Inflammatory effects
• TPN lipid emulsions: Rich in oxidizable lipids and their
oxidation triggers inflammatory response
• Hepatic Steatosis is common with long-term TPN
• Caused by: Chronic overfeeding (carbohydrates + lipids) and
is associated with elevated liver enzymes
• May not represent true pathology
34.
Cholestasis
• Lack ofenteral lipids Reduced cholecystokinin release and
→
hence Gallbladder contraction
↓
• Results in: Bile stasis and Gallbladder sludge
• Can lead to: Acalculous cholecystitis
Bowel Sepsis
• Absence of luminal nutrition causes: Bowel mucosal atrophy
and Impaired gut-associated immunity
• Increases risk of: Systemic spread of enteric pathogens
35.
Peripheral TPN (PPN)
Truncatedform of TPN
• Provides: Protein-sparing nonprotein calories
• Indications:
• Supplement to enteral feeding
• Short-term inadequate nutrition
• Not suitable for: Hypercatabolic patients and malnourished patients
• Osmolarity Requirements - Peripheral infusates with <900 mosm/L
andpH 7.2–7.4
• Requires dilute amino acid and dextrose solutions
• Limits total nutrient delivery
• Isotonic lipids useful to increase nonprotein calories
36.
• Common PPNsolution have 3% amino acids + 20% dextrose
• Final concentration:1.5% amino acids10% dextrose
• Osmolarity:~500 mosm/L
• Caloric content: Dextrose: 340 kcal/L (2.5 L 850 kcal)
→
• Add 250 mL of 20% Intralipid (500 kcal)
• Total nonprotein calories:~1,350 kcal/day
• Adequate for: Average-size, unstressed adult (~20
kcal/kg/day)
37.
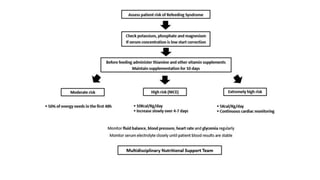
Contraindications
• Patients withcritical cardiovascular instability or metabolic
instabilities; such instabilities require correction before
administering intravenous nutrition.
• Gastrointestinal feeding is possible
• Infants with <8 cm of the small bowel
• Irreversibly decerebrate patients
• Good Nutrition status
• The lack of a therapeutic goal
38.
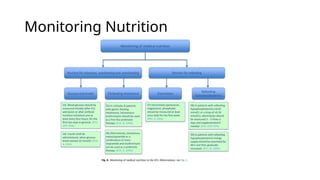
Screening for Malnutrition
•Clinical Assessment
• Nutritional Assessment Score 2002
• Subjective Global Assessment
• Mini Nutritional Assessment
• Assessment of Muscle Mass
• Ultrasound
• Computed Tomography
• Bioelectrical Impedance Analysis
REFEEDING SYNDROME
• Medicalcomplications that result from fluid and electrolyte shifts resulting
from aggressive nutritional rehabilitation.
• high-risk populations
• eating disorders
• chronic alcoholism
• malabsorptive conditions like inflammatory bowel disease,
• chronic malnutrition
• poorly controlled diabetes
• oncological conditions
• post-operative state
41.
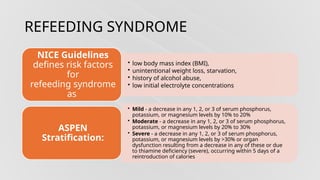
REFEEDING SYNDROME
• lowbody mass index (BMI),
• unintentional weight loss, starvation,
• history of alcohol abuse,
• low initial electrolyte concentrations
NICE Guidelines
defines risk factors
for
refeeding syndrome
as
• Mild - a decrease in any 1, 2, or 3 of serum phosphorus,
potassium, or magnesium levels by 10% to 20%
• Moderate - a decrease in any 1, 2, or 3 of serum phosphorus,
potassium, or magnesium levels by 20% to 30%
• Severe - a decrease in any 1, 2, or 3 of serum phosphorus,
potassium, or magnesium levels by >30% or organ
dysfunction resulting from a decrease in any of these or due
to thiamine deficiency (severe), occurring within 5 days of a
reintroduction of calories
ASPEN
Stratification:
47.
SOURCES
• Chapters –Nutrition and Parentral Nutrition from ICU Book
Paul L Morino
• ESPEN 2023 Guidelines
• ASPEN 2019 Guidelines

![• Actual body weight is used as long as patient is not obese
• If actual body wt is 25% higher than ideal body weight –
adjusted body weight used.
• Adjusted wt (kg) = [(Actual – Ideal) × 0.25] + Ideal wt](https://image.slidesharecdn.com/tpn-260101043945-36560c38/85/TPN-pptx-opppsnkppknippsnppsbipobiopsnkpob-4-320.jpg)
![• Nitrogen Intake
• Protein is 16% nitrogen
• 1g Protein contains 1/6.25 g of Nitrogen
• Nitrogen Intake (g/day) = Protein intake (g/day) / 6.25
• Nitrogen Balance (g/day) - (Protein / 6.25) – [UUN + (4–6)]
GOAL OF NUTRION -positive nitrogen balance of 4–6 grams.](https://image.slidesharecdn.com/tpn-260101043945-36560c38/85/TPN-pptx-opppsnkppknippsnppsbipobiopsnkpob-7-320.jpg)













![Tpn[1]](https://cdn.slidesharecdn.com/ss_thumbnails/tpn1-190610164122-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Reed-Henry]Total-Parenteral-Nutrition.ppt](https://cdn.slidesharecdn.com/ss_thumbnails/reed-henrytotal-parenteral-nutrition-240728195211-676c9b20-thumbnail.jpg?width=640&height=640&fit=bounds)












































