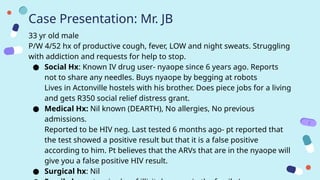
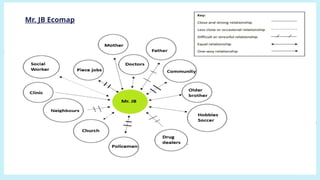
Case Presentation: Mr.JB
33 yr old male
P/W 4/52 hx of productive cough, fever, LOW and night sweats. Struggling
with addiction and requests for help to stop.
● Social Hx: Known IV drug user- nyaope since 6 years ago. Reports
not to share any needles. Buys nyaope by begging at robots
Lives in Actonville hostels with his brother. Does piece jobs for a living
and gets R350 social relief distress grant.
● Medical Hx: Nil known (DEARTH), No allergies, No previous
admissions.
Reported to be HIV neg. Last tested 6 months ago- pt reported that
the test showed a positive result but that it is a false positive
according to him. Pt believes that the ARVs that are in the nyaope will
give you a false positive HIV result.
● Surgical hx: Nil
FRICE
Fears: fears thathe might die of his illness or due to drug use
Reasons: he doesn't seem to get better and only worsens
Ideas: he might have cancer in his lungs
Concerns: worried to be admitted and then withdraw from his
drugs
Expectations: to be healed and helped by the doctors. To be
assisted with his drug addiction
BIO-PSYCHOSOCIAL ASSESSMENT
Biological PsychologicalSocial
33yr old male
Known RVD Not on
treatment
LRTI ?PTB
Substance use disorder
Worried that he might
die from the illness.
Stressed about being
possibly admitted and
then withdraw from
drugs
Misconception about
RVD status
Unemployed- only
piece jobs
Lives In informal
settlement with
younger brother whom
is also an IV drug user
IV drug user
13.
BIO-PSYCHOSOCIAL PLAN
Biological PsychologicalSocial
TB GeneXpert
Defer ARVs once TB
result is available
Start antibiotics for
LRTI
Rehabilitation plan
Reassure the patient
that if he needs to be
admitted we can help
the withdrawals with
methadone. Educate pt
on HIV testing and that
its accuracy is not
affected by nyaope use
Involve social worker to
assist with
unemployment and
rehabilitation program
Involve CHW to trace
pts brother to also test
for TB, HIV and
rehabilitation plan
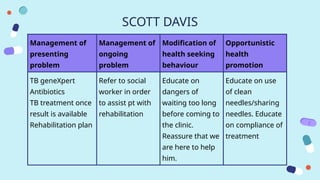
SCOTT DAVIS
Management of
presenting
problem
Managementof
ongoing
problem
Modification of
health seeking
behaviour
Opportunistic
health
promotion
TB geneXpert
Antibiotics
TB treatment once
result is available
Rehabilitation plan
Refer to social
worker in order
to assist pt with
rehabilitation
Educate on
dangers of
waiting too long
before coming to
the clinic.
Reassure that we
are here to help
him.
Educate on use
of clean
needles/sharing
needles. Educate
on compliance of
treatment
INTRODUCTION: SUD
Definition:
According tothe DSM-V, SUD is a complex condition in which there is
uncontrolled use of a substance despite harmful consequences. People with
SUD have an intense focus on using a certain substance to the point where
their ability to function in day-to-day life becomes impaired.
Categories of Substances that are misused or abused
1) Illicit: most common illicit types of substances include cannabis,
amphetamines, ketamine, methamphetamines, cocaine, ecstasy, heroin,
nyaope and mandrax
2) Legal: marijuana, tobacco, alcohol, cough medications, codeine,
psychotropic drugs and benzodiazepines
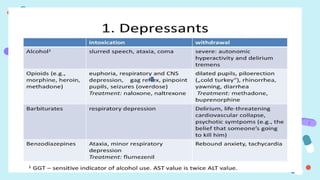
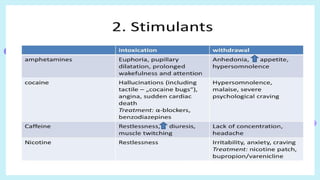
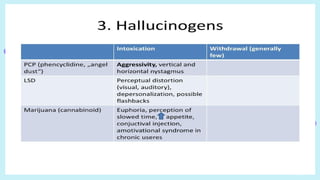
3) These are further categorised into depressants, stimulants and
hallucinogens
History
Basic medical history:Medical, social, family, surgical history
Regarding substance use:
● Type and amount of substance currently using
● How long and to what extend
● Sharing of needles
● How are they accessing the substances? Stealing, begging, etc
● Risk associated- when intoxicated are they aggressive, driving or
abusing partners, homicidal
22.
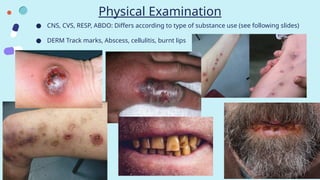
Physical Examination
● CNS,CVS, RESP, ABDO: Differs according to type of substance use (see following slides)
● DERM Track marks, Abscess, cellulitis, burnt lips
24.
Signs & Symptoms
Intoxication:This is the immediate and short-term effect of a
substance in the body. Usually feeling of euphoria
Withdrawal: These are symptoms that happen when the short-term
effects of a substance wear off and the substance starts to leave the
body. Symptoms are unpleasant.
S&S of withdrawal vs intoxication differ according to specific
substance type used such as depressants, stimulants and
hallucinogens
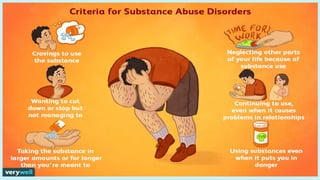
DSM V Criteria
Thesecriteria fall under four basic categories — impaired control, physical dependence,
social problems and risky use:
1. Using more of a substance than intended or using it for longer than you’re meant to.
2. Trying to cut down or stop using the substance but being unable to.
3. Experiencing intense cravings or urges to use the substance.
4. Needing more of the substance to get the desired effect — also called tolerance.
5. Developing withdrawal symptoms when not using the substance.
6. Spending more time getting and using drugs and recovering from substance use.
7. Neglecting responsibilities at home, work or school because of substance use.
8. Continuing to use even when it causes relationship problems.
9. Giving up important or desirable social and recreational activities due to substance
use.
10. Using substances in risky settings that put you in danger.
11. Continuing to use despite the substance causing problems to your physical and
Epidemiology
● The lifetimeprevalence of SUD of the SA population is an estimated 13.3% for at
least one substance.
● The prevalence of substance abuse is more than twice the global average, and the
rates of heavy alcohol drinking are the highest in the world.
● The most commonly abused substance in SA is alcohol, followed by tobacco and
cannabis.
● Amongst young people, inhalant substances are more popular, and cannabis is the
most commonly abused substance, followed by methamphetamine, amphetamine
and heroin.
● An estimated 7% of the population use a narcotic substance during their lifetime.
● Substance abuse is prevalent across all social, racial, cultural, religious and gender
spheres.
● Many research studies have reported the link between substance abuse and various
physical and mental health problems, communicable diseases, intimate partner
violence, child abuse, road traffic accidents and deaths from avoidable causes.
● Treatment, care and rehabilitation of substance abuse place a heavy burden on
overstretched public health systems.
Aetiology
Biological
● Male gender
●Inherited genetic susceptibility to substance abuse
Psychosocial
● Personality traits, for example high impulsivity and aggressive behaviour
● Comorbid mental health conditions, for example major depressive disorder,
anxiety disorder, schizophrenia and post-traumatic stress disorder
● Poor social skills
Contextual
● Parents and a family history of substance abuse
● Peer substance abuse
● Physical, emotional and sexual abuse
● Dysfunctional family
● Accessibility of substances in the community
● Influence of print and online media
Primary Prevention
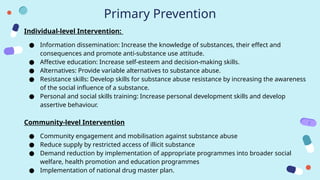
Individual-level Intervention:
●Information dissemination: Increase the knowledge of substances, their effect and
consequences and promote anti-substance use attitude.
● Affective education: Increase self-esteem and decision-making skills.
● Alternatives: Provide variable alternatives to substance abuse.
● Resistance skills: Develop skills for substance abuse resistance by increasing the awareness
of the social influence of a substance.
● Personal and social skills training: Increase personal development skills and develop
assertive behaviour.
Community-level Intervention
● Community engagement and mobilisation against substance abuse
● Reduce supply by restricted access of illicit substance
● Demand reduction by implementation of appropriate programmes into broader social
welfare, health promotion and education programmes
● Implementation of national drug master plan.
40.
Secondary & TertiaryPrevention
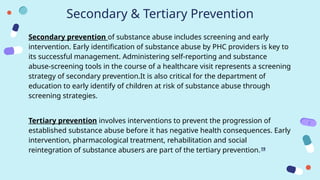
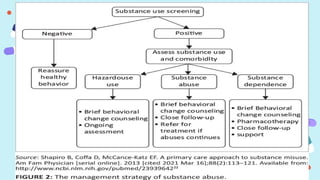
Secondary prevention of substance abuse includes screening and early
intervention. Early identification of substance abuse by PHC providers is key to
its successful management. Administering self-reporting and substance
abuse-screening tools in the course of a healthcare visit represents a screening
strategy of secondary prevention.It is also critical for the department of
education to early identify of children at risk of substance abuse through
screening strategies.
Tertiary prevention involves interventions to prevent the progression of
established substance abuse before it has negative health consequences. Early
intervention, pharmacological treatment, rehabilitation and social
reintegration of substance abusers are part of the tertiary prevention.19
42.
Management
Pharmacological: Plays arole with detoxification, initial recovery, and relapse prevention by
use of pharmacotherapy in order to:
● alleviate withdrawal symptoms
● block euphoric effects or cravings (Naloxone)
● Replace illicit drugs with prescribed medications (Methadone)
● Treat coexisting psychiatric problem (Antidepressants, antipsychotic, etc)
Non-pharmacological
● Psychosocial or psychological interventions: change destructive behaviors, attitudes,
and feelings. They can include individual, group, marital, or family therapy.
● Behavioral therapies: These can help change undesirable behaviors and encourage
desired ones.
● Self-help groups: These can provide mutual support and encouragement to become or
remain abstinent.
43.
Pharmacological Management
1) Alcoholwithdrawal:
Thiamine, oral, 300 mg daily for 14 days AND Diazepam, oral, 10 mg immediately,
Then 5 mg 6 hourly for 3 days, Then 5 mg 12 hourly for 2 days, Then 5 mg daily for 2
days, Then stop.
● Hallucinations and agitation: Haloperidol, oral, 0.75–2.5 mg 12 hourly (Maximum
dose: 5mg per 24 hours)
1) Opioid withdrawal:
Symptomatic treatment Diazepam, oral, 5–20 mg/day in 2-3 divided doses (Taper off
over 5–7 days). Moderate to severe opioid withdrawal- Hospitalise patient.
● Stomach cramps:Hyoscine butylbromide, oral, 20 mg 8 hourly as required.
● Headaches:Paracetamol, oral, 500mg-1 g, 4–6 hourly as required (to a maximum of
4g in 24 hours).
● Muscle pains:NSAID, e.g. Ibuprofen, oral 400 mg 8 hourly, with meals, as required.
● Diarrhoea:Loperamide, oral, 4 mg immediately. Then 2 mg after each loose stool.
44.
Opioid assisted withdrawal:Goal is to safely alleviate withdrawal symptoms without causing intoxication
or overdose.
Day 1: Methadone, oral, 5–10 mg.
If symptoms are still present after 2-4 hour, give another 5–10 mg. Repeat until objective withdrawal
symptoms are adequately managed
Day 2: Methadone, oral.
Repeat total dose of day 1 as a single or 2 divided doses. Monitor for on-going sign and symptoms of
withdrawal.
If the signs and symptoms of withdrawal are still present on day 2, top-up doses of 5 mg may be given at 2–
4
hourly intervals with a total daily dose of up to 30 mg. Consult a person experienced in opioid withdrawal if
symptoms not controlled on 30 mg/day.
Day 3 onwards: Methadone, oral.
Repeat total dose of day 2 if top-ups were needed and begin reductions on the following day (e.g. day 4). If no
top-ups required on the previous day (e.g. day 2) and withdrawal symptoms are adequately controlled, begin
dose reduction. Decrease dose by 10–20% per day over a period of 3–10 days. The withdrawal regimen may
be shortened, if the patient’s withdrawal symptoms allow it.
If methadone is unavailable:
● Tramadol, oral, 200 mg 12 hourly for 14 days may attenuate withdrawal symptoms.
45.
Referral
● All patientstreated for substance withdrawal should be referred to Social Services
and/or a rehabilitation service for management of their substance use and
aftercare.
● Discuss those with comorbid mental disorders with a psychiatrist; refer to specialist
dual diagnosis services where available.
● Family and/or partners of people who use substances to registered counsellors
and support groups (e.g., Al-anon family groups)
Tintswalo: Community Outreach team that assist people with substance use
disorder
● Members found at Actonville police station every Monday
● Opioid assisted withdrawal using methadone
● Clean needle and syringes campaign
● Reintegration into society
● Social worker involvement in order to assist with family relationships
● Admission into rehabilitation centres
Conclusion
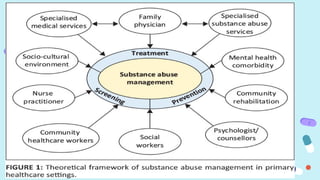
● Primary careis the right place for routine screening and management of
substance abuse.
● Substance abuse management within the context of primary care could
increase access to and retention in care and improve health outcomes.
● The integrated care of substance abuse management can reduce the
overall costs of healthcare.
● Specialist guidance in the coordinated care of substance abuse services in
primary care settings can improve the continuum of healthcare.
● Similar to other chronic illnesses, substance abuse can be efficiently
managed by PHC providers in a primary care structure by a brief
behavioural counselling and medication.
● Indeed, the strength of primary care is in the use of PHC providers’ skills
to address the broad range of healthcare issues related to substance
abuse.
● US Departmentof Health and Human Services; 2016 Nov. CHAPTER 7, VISION
FOR THE FUTURE: A PUBLIC HEALTH APPROACH. Available from:
https://www.ncbi.nlm.nih.gov/books/NBK424861/
● Lo TW, Yeung JWK, Tam CHL. Substance Abuse and Public Health: A Multilevel
Perspective and Multiple Responses. Int J Environ Res Public Health. 2020 Apr
10;17(7):2610. doi: 10.3390/ijerph17072610. PMID: 32290248; PMCID:
PMC7177685.
● Myers, B., Koch, J.R., Johnson, K. et al. Factors associated with patient-reported
experiences and outcomes of substance use disorder treatment in Cape Town,
South Africa. Addict Sci Clin Pract 17, 8 (2022).
https://doi.org/10.1186/s13722-022-00289-3
● https://www.gov.za/Alcoholandsubstanceabuse
● https://www.gov.za/sites/default/files/gcis_document/201409/32150436.pdf
● Kaswa R. Primary healthcare approach to substance abuse management. S Afr Fam
Pract. 2021;63(1), a5307. https://doi.org/10.4102/safp.v63i1.5307
● Department of Family Medicine and Rural Health, Walter Sisulu University, Mthatha,
South Africa
50.
CREDITS: This presentationtemplate was
created by Slidesgo, including icons by Flaticon
and infographics & images by Freepik
Thanks
Do you have any questions?
Please keep this slide for attribution


















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)













