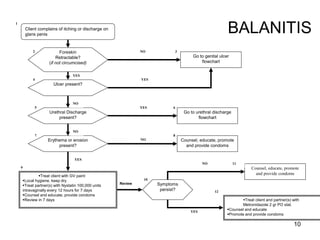
1. The document contains flowcharts for diagnosing and managing various sexually transmitted infections (STIs) such as urethral discharge, abnormal vaginal discharge, genital ulcers, lower abdominal pain, and balanitis.
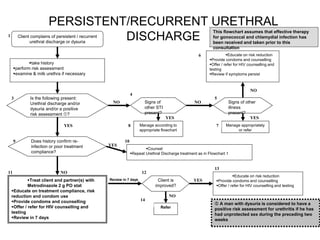
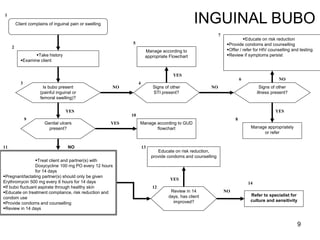
2. The flowcharts provide guidance on taking a patient history, performing physical examinations, assessing risk factors, making diagnoses, and treating patients and their partners with recommended antibiotics or antivirals.
3. Education is emphasized throughout, including educating patients on risk reduction, condom use, treatment compliance, and offering HIV counseling and testing. Follow-up reviews are also recommended to monitor for improvement.