Downloaded 25 times

![In the news
Novopay a $30m horror show
‘… such rush-jobs are all too common … [the
government] may be setting the stage for future
horrors with its stated policy of getting a national
patient-record system in place by 2014’
Sunday Star Times, 25/11/12](https://image.slidesharecdn.com/orionhealthcarecollaborativestandardsandinteroperabilityfor2014nov2012v1-0-121217010530-phpapp02/75/Standards-and-interoperability-towards-2014-and-the-New-Zealand-e-health-vision-3-2048.jpg)
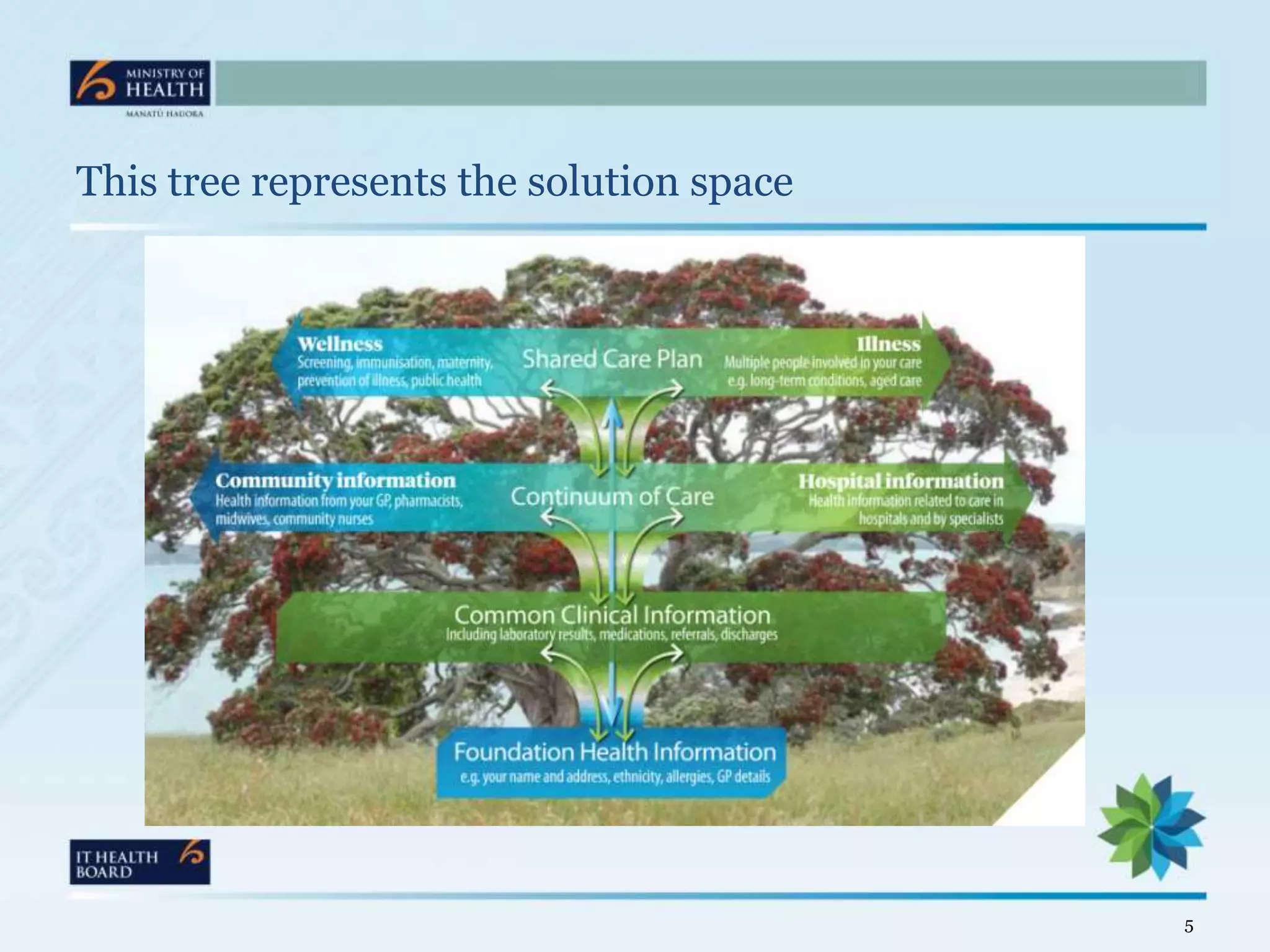
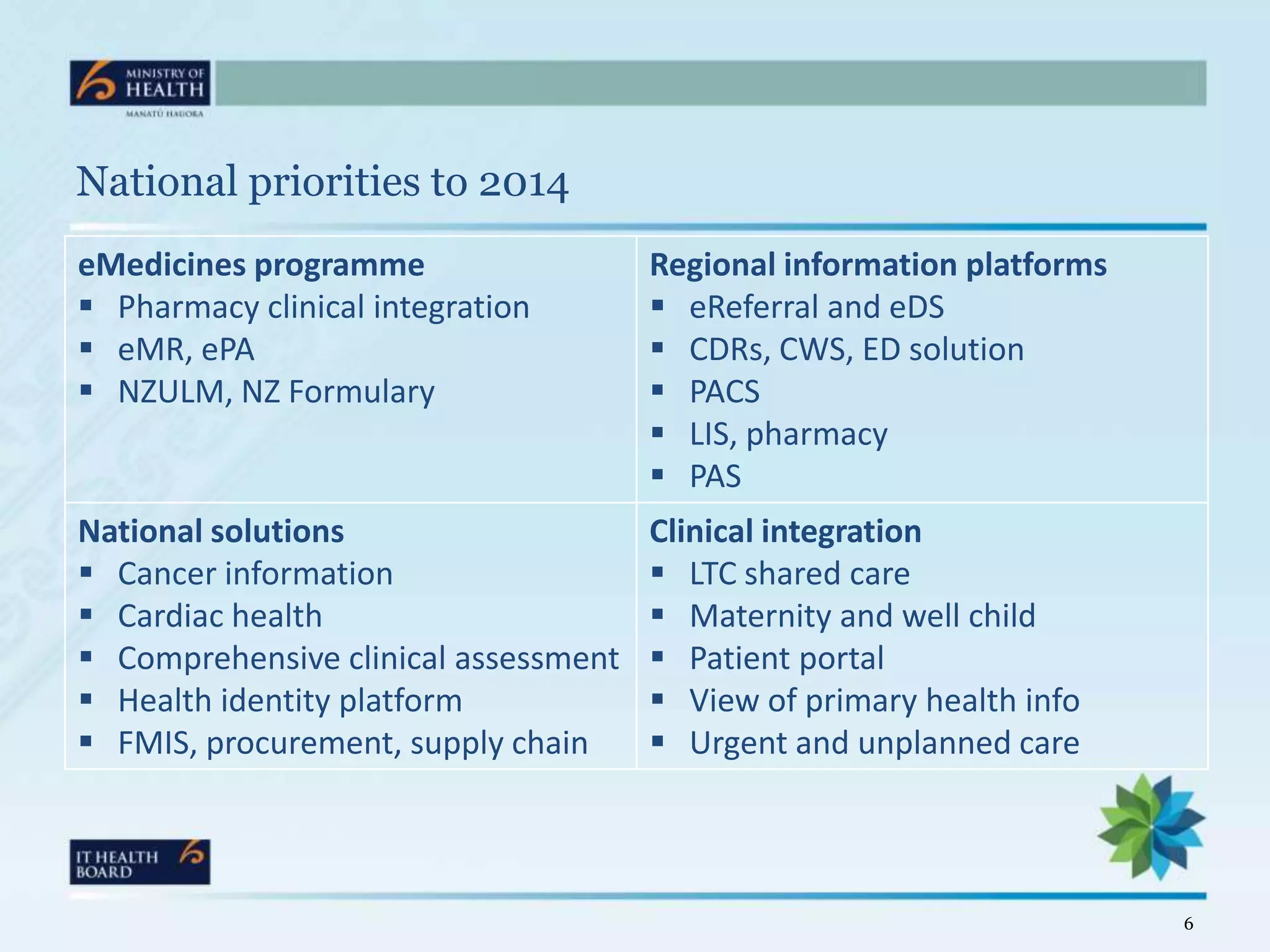







The document discusses New Zealand's healthcare integration strategy aimed at achieving person-centred care by 2014, focusing on shared care among clinicians and the use of technology. It highlights the importance of national priorities, clinical integration, and the development of regional information platforms to improve patient care. Challenges include the transition to electronic medical records and the need for standardized processes across healthcare systems.


















































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)





