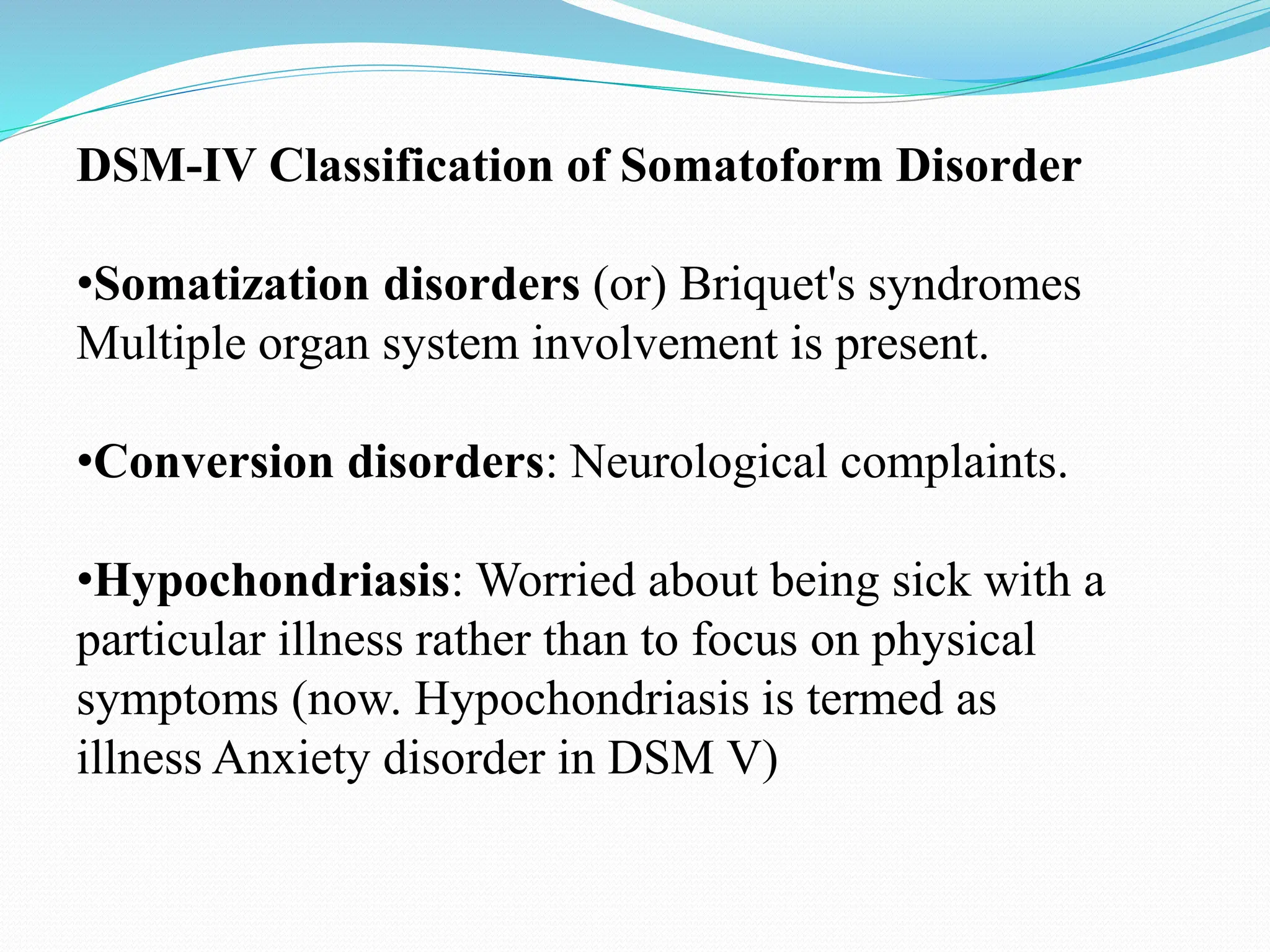
This document discusses somatoform disorders and dissociative disorders. It defines somatoform disorders as mental illnesses where patients experience physical symptoms that cannot be explained medically. It outlines the DSM-IV and DSM-V classifications of somatoform disorders including somatic symptom disorder. Dissociative disorders involve lack of connection in consciousness and identity. Dissociative disorders discussed include dissociative amnesia, dissociative fugue, and dissociative identity disorder. Treatment options mentioned include various forms of psychotherapy and drug therapy.