Skin systemic infections final
•
1 like•638 views

Cutaneous manifestations of systemic infections can include: 1. Osler nodes and Janeway lesions in infective endocarditis, appearing as tender nodules on fingers or palms. 2. Rashes caused by viral exanthems like measles, rubella, enteroviruses. Measles causes Koplik's spots. 3. Fungal infections in immunocompromised patients like candidiasis, dermatophytosis, cryptococcus causing papules or plaques. 4. Bacterial infections may cause cellulitis, ecthyma gangrenosum from Pseudomonas, or disseminated lesions in meningococcemia.

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Skin systemic infections final
Similar to Skin systemic infections final (20)
More from DR RML DELHI
More from DR RML DELHI (20)
Recently uploaded
Recently uploaded (20)
Skin systemic infections final
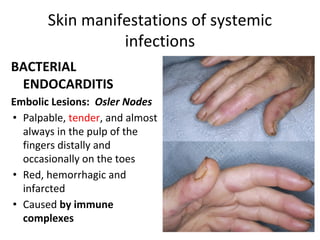
- 1. Skin manifestations of systemic infections BACTERIAL ENDOCARDITIS Embolic Lesions: Osler Nodes • Palpable, tender, and almost always in the pulp of the fingers distally and occasionally on the toes • Red, hemorrhagic and infarcted • Caused by immune complexes
- 2. Janeway Lesions • Red, macular, papular, infarctive,nontender, and almost always on the palms or soles; usually part of the vasculitis of SBE • caused by vascular phenomenon
- 4. • Subungual Splinter Hemorrhages • Septic embolic phenomenon. • Linear in the middle of the nailbed in acute IE (Distal hemorrhages are traumatic.) Common in acute S. aureus IE. • Petechial Lesions Small, nonblanching, reddish-brown macules. Occur on extremities, upper chest, mucous membranes
- 5. Cutaneous Manifestations and Characteristics of Infective Endocarditis Cutaneous Manifestations Palpation Morphologic Findings Osler node Tender Erythematous papules and nodules with white centers; may become necrotic Janeway lesions Nontender Hemorrhagic papules Splinter hemorrhages Nontender Subungual hemorrhagic streaks
- 6. anthrax • Greek word,meaning coal • Gram positive rod,bacillus anthracis • painless papule that evolves into a hemorragic bulla with surrounding brawny non-pitting edema
- 7. CLASSIFICATION OF CUTANEOUS TUBERCULOSIS Exogenous inoculation: Skin inoculation • Primary inoculation tuberculosis (PIT), i.e., tuberculous chancre: occurs at inoculated site in nonimmune host. • Metastatic tuberculosis abscess (MTA) • Acute miliary tuberculosis (AMT) • Orificial tuberculosis (OT) Tuberculosis due to BCG immunization
- 8. • Tuberculosis Verrucosa Cutis • Initial papule with violaceous halo. Evolves to hyperkeratotic,warty, firm plaque. Clefts and fissures occur from which pus and keratinous material can be expressed. Border often irregular. • Lesions are usually single, but multiple lesions may occur. Most commonly on dorsolateral hands and fingers. In children, lower extremities,knees. No lymphadenopathy.
- 9. • Lupus Vulgaris.. • Hypertrophic forms result in soft tumorous nodules. • Ulcerative forms present as punched-out, often serpiginous ulcers surrounded by soft, brownish infiltrate. Usually solitary, but several sites may occur. Most lesions on the head and neck, most often on nose and ears or scalp.
- 10. • Scrofuloderma • Firm subcutaneous nodule that initially is freely movable; lesion then becomes doughy and evolves into irregular,deep-seated node or plaque that liquefies and perforates . • Ulcers and irregular sinuses, usually of linear or serpiginous shape, discharge pus or caseous material. • Most often occurs in the parotidal, submandibular,and supraclavicular regions; • SD most often results from contiguous spread from affected lymph nodes or tuberculous bones (phalanges, sternum, ribs) or joints.
- 11. • Metastatic Tuberculosis Abscess • Also called tuberculous gumma . Subcutaneous abscess,nontender, “cold,” fluctuant. Coalescing with overlying skin, breaking down and forming fistulas and ulcers. Single or multiple lesions, often at sites of previous trauma. • Acute Miliary Tuberculosis Exanthem. • Disseminated lesions are minute macules and papules or purpuric lesions. Sometimes vesicular and crusted. Removal of crust reveals umbilication.Disseminated on all parts of body, particularly trunk.
- 12. tuberculids • Demonstratable tuberculosis focus,no acid fast bacilli in the skin lesions,strong Montoux test and tuberculoid granuloma on biopsy • It includes- I. Erythema induratum II. Papulonecrotic tuberculid III. Lichen scrofulosorum IV. Erythema nodosum
- 13. • Erythema induratum:tender nodules and ulcers over calves of young ladies
- 14. • The lesions appear as small firm follicular brownish pinhead papules that occur symmetrically on the limbs, mainly on the extensor surface, trunk and face • Central necrosis of the lesions may follow, ending with small-pitted scars
- 15. • Lichen scrofulosorum • The lesion occurs over the trunk mainly in children having tuberculosis of the bone or lymph nodes. • Skin presents with firm, flat-topped hyperkeratotic papules surmounted by pustule or tiny scales, arranged in groups and have a very chronic course. • The lesions may undergo spontaneous involution and may recur again.
- 16. • Erythema nodosum : tender,erythematous nodules and plaques over shins
- 17. septicaemia • Septic vasculitis: there may be palpable purpura,haemorrhag ic vesicles,skin infarcts
- 18. Disseminated intravascular coagulation (DIC) is • a widespread blood clotting disorder • Manifested by purpura fulminans (cutaneous infarctions and/or acral gangrene) or bleeding from multiple sites.
- 19. • Meningococcaemia: • Neisseria meningiditis • palpable purpura with hemorrhagic vesicles are present over limbs
- 20. Pseudomonas septicaemia:necrotic ulcers with yellow green discharge Ecthyma gangrenosum (EG) is the necrotizing soft tissue infection that occurs after local tissue invasion or bacteremic seeding, associated with blood vessel invasion, septic vasculitis, vascular occlusion, and infarction of tissue.
- 21. Viral infections 1. Viremia due to many viruses:maculopapular or papulovesicular exanthem and enanthem 2. Hepatitis B:cutaneous vasculitis
- 22. measles • Rubeola [measles] • paramyxovirus Koplik’s spots • Behind the ear,hairline,forehead • Atypical measles
- 23. Koplik’s spots
- 24. • RUBELLA • “little red” • Toga virus • German measles • Retroauricular lympadenopathy • Suboccipetal lymphadenopathy
- 25. ERYTHEMA INFECTIOSUM • Parvovirus B19 • Erythema of cheeks followed by reticulated pattern on extremities
- 26. • Rubelliform and roseoliform eruptions also seen in • Epstein barr virus • Echovirus • Coxsackievirus • Cytomgalovirus • Adenovirus • Denguevirus • West Nile virus
- 27. Scarlet fever • Beta hemolytic streptococcal infection • Scarlantiform(confluent blanching erythema) • White strawberry tongue • Red strawberry tongue
- 28. Kawasaki disease(mucocutaneous lymph node syndrome) • Morbilliform and scarlanitiform • b/l conjunctival injection,erythema and edema of hands and feet f/b desquammation • Diffuse erythema of oropharynx,red strawberry tongue,dry fissured lips
- 30. HIV • Cutaneous Signs Of Primary HIV Infection Macularerythematous lesions on the trunk, roseola-like or morbilliform eruptions in the upper body or face • and papulosquamous manifestations of the palms and soles
- 31. Secondary Mucocutaneous Signs Of HIV Infection • Viral Infections:Herpes simplex • a recurrent self-healing blistering eruption may occur at any stage of HIV infection • Erosions enlarges and deepen into painful, non-healing ulcers
- 32. Varicella-Zoster • can occur at any stage of HIV disease • in the majority a typical a vesicular eruption in a dermatomal pattern • some cases develop severe haemorrhagic and necrotic lesions that may extend over several dermatomes, and eventually disseminate all over the body
- 33. Molluscum Contagiosum • include skincoloured umbilicated papules with one or more central hyperkeratotic pores • commonly on the face , genital regions • Widespread lesions are common and highly characteristic of HIV disease
- 34. Human Papillomavirus (HPV) • incidence of facial and intraoral warts is increased and anogenital lesions may be florid
- 35. Fungal infections in HIV • Cryptococcus neoformans-painless reddish papules and nodules • Histoplasma capsulatum- widespread maculopapular rash, necrotic papules and ulcers • Sporotrix schenkii-papulonodular eruptions • Candida spp, Dermatophytes and Malassezia furfur infections are the most common pathogens responsible for superficial mycoses in HIV infected patients.
- 36. • Histoplasma capsulatum- widespread maculopapular rash, necrotic papules and ulcers
- 37. Candidiasis • most common cause of fungal infections • Candida albicans,C. tropicalis, C. kruzei and C.glabrata • may affect both oral mucosa and skin • Skin involvement includes intertrigo, folliculitis, paronychia, and/or onychomycosis
- 38. Oropharyngeal candidiasis • 4 patterns- • l) pseudomembranous (thrush) characterized by whitish or yellowish plaques within the oral cavity; • 2) erythematous or atrophic, characterized by bright red erosions or ulcers within the oral cavity; • 3) hyperplastic, characterized by exuberant yellowish-whitish plaques • 4)angular cheilitis, characterized by crusting, fissuring and erythema at the angles of the mouth
- 39. Dermatophyte Infections • chronic and unusually widespread, and the morphology may be altered by enhancement or diminuition of the inflammatory component • Nail involvement is common often affecting all finger nails and toe nails, may occur in an unusual form featuring proximal whitening of nail plate
- 40. Pityriasis Versicolor • Malassezia furfur • pityriasiform desquamation and hypopigmented or hyperpigmented macules formation, primarily located on the chest and back with tendency to spread • unusually extensive and persistent in advanced immunosuppression
- 41. scabies • Crusted (Norwegian) scabies in which the number of infesting mites can increase enormously • generalized scaling-to-marked hyperkeratosis
- 42. Kaposi's Sarcoma • Skin lesions include red, purplish or brown coloured macules, nodules or plaque • Any part of the body surface may be affected but • common sites are trunk, legs, face and oral cavity
- 43. Miscellaneous Disorders associated with HIV • Seborrhoeic Dermatitis • Psoriasis Vulgaris • Reiter’s Syndrome • Ichthyosiform Dermatosis • Papular/Pruritic Eruptions • Eosinophilic Folliculitis • Adverse Cutaneous Drug Reactions • Oropharyngeal candidiasis • Oral Hairy Leucoplakia • Aphtous Ulcers
- 44. Syphilis• Primary syphilis:initial lesion,called chancre,evolve after 3-90 days of exposure • classically (40% of the time) a single, firm, painless, non-itchy skin ulceration with a clean base and sharp borders between 0.3 and 3.0 cm in size • multiple lesions may be present (~40%),more common when coinfected with HIV • may be painful or tender (30%), and they may occur outside of the genitals (2–7%) • most common location (in women) cervix (44%), penis in heterosexual men (99%), and anally and rectally relatively commonly in homosexual men (34%) • lesionmay persist for three to six weeks without treatment
- 45. • Secondary syphilis occurs approximately four to ten weeks after the primary infection • commonly involve the skin, mucous membranes, and lymph nodes. • There may be a symmetrical reddish-pink non-itchy rash on the trunk and extremities, including the palms and soles. The rash may become maculopapular or pustula r. It may form flat, broad, whitish, wart-like lesions known as condyloma latum on mucous membranes
- 46. Leptospirosis • Red, irregular blotches appear on the skin that are dark red in color, sometimes turning a purple hue. They can appear anywhere on the body but are often seen on the lower legs and the palatte • Do not blanch on pressure
- 47. Fungaemia • Cryptococcosis: • Papules,nodules and ulcers over face and limbs are seen
- 48. • Histoplasmosis: Papules or nodules; erythematous, necrotic, • or hyperkeratotic • Erythematous macules; scaling
- 49. Parasitic infestations • Post kala-azar dermal leishmaniasis: • Sequel to VL • Lesions appear ≥1 y after course of therapy with macular,papular, nodular lesions, and hypopigmented macules/plaques on face, trunk, extremities.
- 50. • Cysticercosis: • May present as asymptomatic subcutaneous nodules over trunk