
Recommended
Recommended
More Related Content
Similar to Sigmoid sinus thrombosis in otolaryngology
Similar to Sigmoid sinus thrombosis in otolaryngology (20)
Recently uploaded
Recently uploaded (20)
Sigmoid sinus thrombosis in otolaryngology
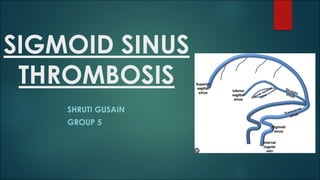
- 2. What is Sigmoid Sinus Thrombosis ? u Lateral sinus thrombosis ,also known as sigmoid sinus thrombosis forms when infection from the adjacent mastoid contacts and penetrates the venous wall and forms a thrombus. u SST Is a rare but serious medical condition that occurs when a blood clot forms in the sigmoid sinus, a large vein located at the base of the brain that drains blood from the brain. u The clot can block blood flow and lead to a buildup of press In brain and cause relative symptoms . u Embolisation of the thrombus can cause distal disease
- 3. Etiology ? u Genetic prothrombotic conditions: -Antithrombin deficiency, Protein C and protein S deficiency, Factor V Leiden mutation, Prothrombin mutation (the substitution of A for G at position 20210), homocysteinemia caused by gene mutations in methylenetetrahydro-folate reductase. u Acquired prothrombotic states: Nephrotic syndrome, Antiphospholipid antibodies, Homocysteinemia, Pregnancy, Puerperium. u Infections: Otitis, mastoiditis, sinusitis, Meningitis, Systemic infectious disease. u Inflammatory disease: Systemic lupus erythematosus, Wegener's granulomatosis, Sarcoidosis Inflammatory bowel diseases, Behçet's syndrome u Hematologic conditions: Polycythemia, primary and secondary ThrombocythemiaLeukemia , anemia, including paroxysmal nocturnal hemoglobinuria . u Drugs: Oral contraceptives ,Asparaginase u Mechanical causes, trauma u Miscellaneous: Dehydration, especially in children , Cancer.
- 4. Anatomy & Spread ? u Formed by the confluence of the superior petrosal and transverse sinuses . u Becomes internal jugular vein at its exit from foramen jugulare. u Directly through bone erosion due to granulation and cholesteatoma. u Thrombophlebitis of the mastoid emissary veins. • Griesinger’s Sign – erythema , edema and tenderness over mastoid area.
- 6. Epidemiology u Age – ADULTS OR OLDER CHILDREN u 6- 10 % of all Intracranial complication of chronic otitis media. u Types of ear infections associated- most common with cholesteatoma. Ø May occur from other forms of chronic mastoiditis. Ø Acute otitis media in rare cases – caused by osteothromophlebitis. § Other associated intracranial complications- meningitis, epidural abscess, subdural empyema , cerebellar abscess.
- 12. Clinical features: u In the era of antibiotics, may be present without symptoms • Classical presentation is very rare- components were: 1. There was severe febrile illness with rigors in patient with middle ear disease. 2. Rise of temperature to 39-40 c and rapid fall of temperature with sweating( picket fence fever pattern due to periodic release of streptococci in blood from septic thrombus. 3. Shivering used to be so severe so as to shake the bed. 4. Headache and neck pain ( due to incr. ICP —>papilledema ). 5. Anaemia with emaciation was also seen in classical cases.
- 13. Clinical features: o Feeling of being ill. o Persistent fever ( but without violent swings and rigors as seen in pre antibiotic era) . o Headache, vomiting( due to raise ICP and bacteremia ). o Otalgia with mastoid tenderness . o Neck pain, Neck torticollis along with tenderness along jugular vein. o When thrombosis extend to subclavian vein -engorged collateral veins over shoulder maybe seen. o development of hydrocephalus o Chemosis or proptosis of one eye o drowsiness, lethargy, coma
- 14. Examination Findings? u Otoscopic findings suggestive of middle ear infections. u Tenderness over mastoid process and sternomastoid . u Fundus examination- Papilloedema . u Griesingers sign - pitting edema over the occipital region well behind the mastoid process caused by clotting within large mastoid emissary vein. u Anemia and emaciation u Positive Tobey- Ayer’s Test. u Positive Crow- Beck’s Test. u Kernig’s and Brudzinski’s Sign.
- 16. Bacteriology & Labs u ACUTE o Hemolytic streptococcus o Pneumococci o Staphylococci u CHRONIC o Bacillus Proteus o Pseudomonas pyocyaneus o E.coli o Bacteroides o Staphylococci u Increase Polyp on CBC. u CSF exam show increased ICP. u Lumbar puncture should be performed if papilloedema does not suggest that raised intra cranial pressure may lead to coming. u CSF analysis done in cases of suspected meningitis.
- 21. Treatment? u Medical + Surgery —à combination therapy u Medicine: • I/V antibiotics • Anticoagulant only if clot in superior sagittal sinus or increased ICP persists despite medical management.
- 22. u Surgical: o Mastoidectomy + removal of clot from sinus. o ASOM - Cortical + removal of sinus plate. o CSOM + Cholesteatoma : radical o Refractory Septicaemia: UV litigation to stop emboli being thrown into circulation. ü Follow up: - o Post op antibiotic for 2- 3 weeks o Post op MRI & MRV.
- 23. Complications? Ø Complications of sigmoid sinus thrombosis may include: ü Increased pressure in the brain: Sigmoid sinus thrombosis can cause an increase in intracranial pressure, which can lead to headaches, nausea, vomiting, and changes in vision. ü Neurological deficits: Depending on the location and extent of the clot, sigmoid sinus thrombosis can cause neurological deficits, such as weakness, numbness, or paralysis on one side of the body. ü Hearing loss: Sigmoid sinus thrombosis can affect the inner ear and cause hearing loss or ringing in the ears. ü Seizures: In some cases, sigmoid sinus thrombosis can lead to seizures, which can cause sudden, uncontrolled movements and loss of consciousness. ü Meningitis: Sigmoid sinus thrombosis can lead to the development of meningitis, which is a serious infection that can cause inflammation of the brain and spinal cord. ü Pulmonary embolism: In rare cases, a blood clot from the sigmoid sinus can break off and travel to the lungs, causing a pulmonary embolism.
- 24. Case study u A 35-year-old woman presented to the emergency department with a severe headache that had been ongoing for the past two days. She had no significant medical history and was not taking any medications. On examination, she had a fever of 38.5°C and was sensitive to light. She also had tenderness over the left ear. u A CT scan of the head showed no abnormalities, but a subsequent MRI with contrast revealed a thrombus in the left sigmoid sinus. The patient was diagnosed with sigmoid sinus thrombosis and was started on intravenous antibiotics and anticoagulation therapy. u Over the next few days, the patient's symptoms gradually improved, and she was discharged from the hospital on oral anticoagulation therapy. A follow-up MRI after six months showed resolution of the thrombus. u Although the exact cause of the thrombus was not determined, the patient reported having a recent upper respiratory tract infection, which may have contributed to the development of the clot. The patient was advised to seek medical attention immediately if she experienced any recurrent symptoms.
- 25. Links to additional videos u https://youtu.be/Ip4xT4DQ0U4 u https://youtu.be/v7wiFiHzaEU u https://youtu.be/qMpXDbcLX9o u https://youtu.be/SZKTnrHmS4I