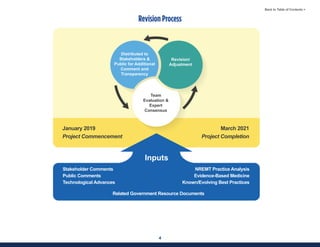
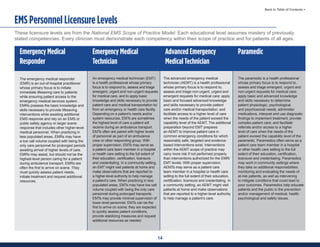
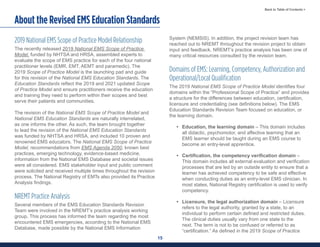
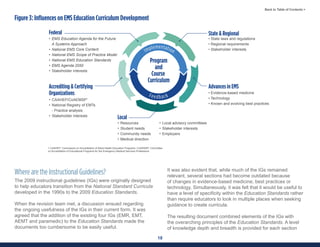
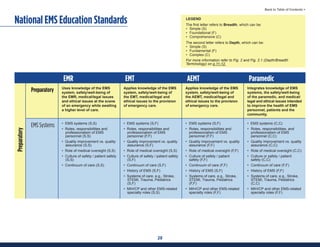
This document summarizes the 2021 National EMS Education Standards. It outlines key inputs that were considered in revising the standards, including stakeholder comments, best practices, technological advances, and evidence-based medicine. Notable revisions were made to standards regarding public health, pediatrics, geriatrics, behavioral health, cultural humility, EMS operations, pharmacology, and EMS safety/wellness. The standards define minimum competencies for entry-level EMS clinicians based on the National EMS Scope of Practice Model. They are designed to allow for diverse implementation methods while ensuring clinicians are competent in their scope of practice.















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

