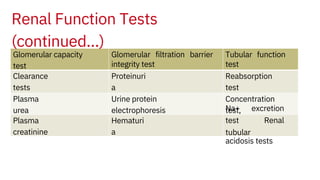
This document discusses assessment of renal function through various tests. It begins by explaining the two main functions of the kidneys - formation of urine and production of hormones. It then describes the process of urine formation and defines three groups of renal function tests: tests of glomerular filtration capacity, tests of the glomerular filtration barrier integrity, and tests of tubular function. Specific tests are discussed in detail including clearance tests, plasma creatinine, proteinuria, concentration tests, and sodium excretion tests. Interpretation of results for evaluating renal function is provided.