Objectives
- Define refractoryepilepsy.
- Understand its epidemiology and causes.
-pathophysiology.
- Discuss the diagnostic criteria and challenges.
-Management
- Review current treatment options.
-conclusion.
Epidemiology
- Epilepsy affectsapproximately 50 million
people worldwide.
- Around 30% of patients with epilepsy are drug-
resistant.
- Higher prevalence in individuals with structural
or genetic predispositions.
6.
Causes and RiskFactors
- Causes:
• Structural abnormalities (e.g., cortical dysplasia,
old stroke,tumors).
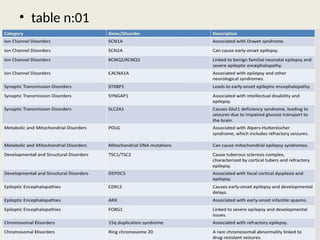
• Genetic factors (e.g., Dravet syndrome ,
other see table 1).
• Metabolic and immune-related causes(see table 2).
• Infectious causes :
(e.g. meningaitis , neurocysticercosis).
- Risk Factors:
• Early onset of seizures..
• High seizure frequency before treatment.
• Inappropriate initial therapy.
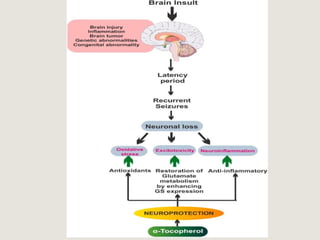
Altered Excitatory-Inhibitory
Balance NetworkReorganization
- Epileptogenesis: Formation of
hyperexcitable networks.
- Synaptic plasticity changes enhance
seizure propagation.
Pathophysiology
- Overactivation of excitatory glutamate
receptors (NMDA, AMPA).
- Impaired GABAergic inhibition due to
receptor dysfunction or interneuron loss.
10.
physiopathology
Cellular and MolecularFactors Neuronal Damage
- Recurrent seizures lead to neuronal
injury, perpetuating a cycle of
resistance.
- Inflammatory mediators (e.g.,
cytokines) contribute to
hyperexcitabili
- Ion channel mutations
(e.g., Na+, K+, Ca2+ channels).
- Increased expression of drug-efflux
transporters (e.g., P-glycoprotein).
12.
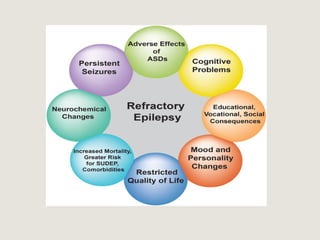
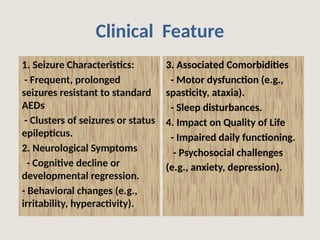
3. Associated Comorbidities
-Motor dysfunction (e.g.,
spasticity, ataxia).
- Sleep disturbances.
4. Impact on Quality of Life
- Impaired daily functioning.
- Psychosocial challenges
(e.g., anxiety, depression).
Clinical Feature
1. Seizure Characteristics:
- Frequent, prolonged
seizures resistant to standard
AEDs
- Clusters of seizures or status
epilepticus.
2. Neurological Symptoms
- Cognitive decline or
developmental regression.
- Behavioral changes (e.g.,
irritability, hyperactivity).
13.
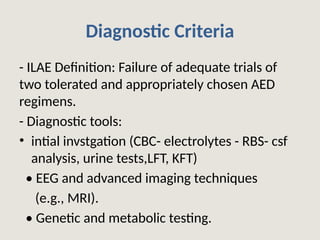
Diagnostic Criteria
- ILAEDefinition: Failure of adequate trials of
two tolerated and appropriately chosen AED
regimens.
- Diagnostic tools:
• intial invstgation (CBC- electrolytes - RBS- csf
analysis, urine tests,LFT, KFT)
• EEG and advanced imaging techniques
(e.g., MRI).
• Genetic and metabolic testing.
14.
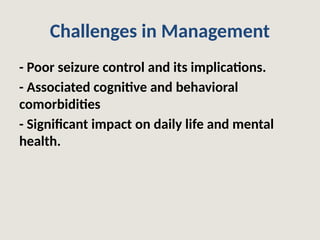
Challenges in Management
-Poor seizure control and its implications.
- Associated cognitive and behavioral
comorbidities
- Significant impact on daily life and mental
health.
15.
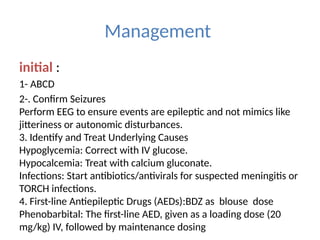
Management
initial :
1- ABCD
2-.Confirm Seizures
Perform EEG to ensure events are epileptic and not mimics like
jitteriness or autonomic disturbances.
3. Identify and Treat Underlying Causes
Hypoglycemia: Correct with IV glucose.
Hypocalcemia: Treat with calcium gluconate.
Infections: Start antibiotics/antivirals for suspected meningitis or
TORCH infections.
4. First-line Antiepileptic Drugs (AEDs):BDZ as blouse dose
Phenobarbital: The first-line AED, given as a loading dose (20
mg/kg) IV, followed by maintenance dosing
17.
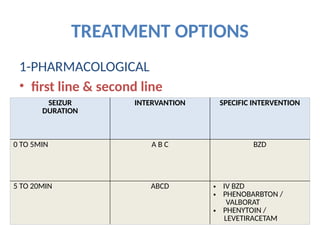
TREATMENT OPTIONS
1-PHARMACOLOGICAL
• firstline & second line
SEIZUR
DURATION
INTERVANTION SPECIFIC INTERVENTION
0 TO 5MIN A B C BZD
5 TO 20MIN ABCD • IV BZD
• PHENOBARBTON /
VALBORAT
• PHENYTOIN /
LEVETIRACETAM
18.
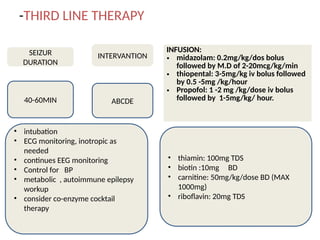
-THIRD LINE THERAPY
SEIZUR
DURATION
INTERVANTION
40-60MINABCDE
INFUSION:
• midazolam: 0.2mg/kg/dos bolus
followed by M.D of 2-20mcg/kg/min
• thiopental: 3-5mg/kg iv bolus followed
by 0.5 -5mg /kg/hour
• Propofol: 1 -2 mg /kg/dose iv bolus
followed by 1-5mg/kg/ hour.
• intubation
• ECG monitoring, inotropic as
needed
• continues EEG monitoring
• Control for BP
• metabolic , autoimmune epilepsy
workup
• consider co-enzyme cocktail
therapy
• thiamin: 100mg TDS
• biotin :10mg BD
• carnitine: 50mg/kg/dose BD (MAX
1000mg)
• riboflavin: 20mg TDS
19.
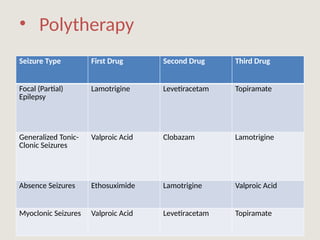
• Polytherapy
Seizure TypeFirst Drug Second Drug Third Drug
Focal (Partial)
Epilepsy
Lamotrigine Levetiracetam Topiramate
Generalized Tonic-
Clonic Seizures
Valproic Acid Clobazam Lamotrigine
Absence Seizures Ethosuximide Lamotrigine Valproic Acid
Myoclonic Seizures Valproic Acid Levetiracetam Topiramate
20.
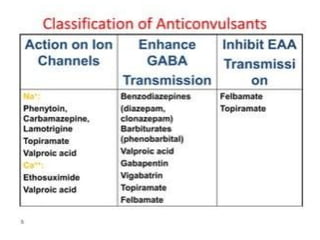
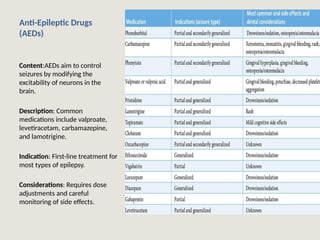
Anti-Epileptic Drugs
(AEDs)
Content:AEDs aimto control
seizures by modifying the
excitability of neurons in the
brain.
Description: Common
medications include valproate,
levetiracetam, carbamazepine,
and lamotrigine.
Indication: First-line treatment for
most types of epilepsy.
Considerations: Requires dose
adjustments and careful
monitoring of side effects.
21.
• No pharmacological
AdvancedTherapies for Refractory Seizures
- Dietary therapies
(e.g., ketogenic diet).
- Neurostimulation
(e.g., vagus nerve stimulation).
- Surgical Options:
Resective surgery
and palliative surgeries
(e.g., corpus callosotomy)
-Immunomodulatory Therapy.
-Corticosteroids.
- Plasma Exchange.
22.
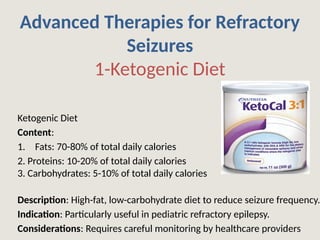
Advanced Therapies forRefractory
Seizures
1-Ketogenic Diet
Ketogenic Diet
Content:
1. Fats: 70-80% of total daily calories
2. Proteins: 10-20% of total daily calories
3. Carbohydrates: 5-10% of total daily calories
Description: High-fat, low-carbohydrate diet to reduce seizure frequency.
Indication: Particularly useful in pediatric refractory epilepsy.
Considerations: Requires careful monitoring by healthcare providers
23.
2-Vagus Nerve Stimulation(VNS)
Content: VNS is a medical treatment that involves
delivering electrical impulses to the vagus nerve.
Description: Implantable device that sends electrical
impulses to the vagus nerve.
Indication: For drug-resistant epilepsy.
Considerations: Surgery required; side effects include
hoarseness.
24.
3-Responsive Neurostimulation (RNS)
ResponsiveNeurostimulation (RNS)
Description: Device that monitors and responds to
brain activity in real-time.
Indication: Intractable focal epilepsy.
Considerations: Involves surgery; results may vary.
25.
4-Surgical Resection
Surgical Resection
Description:Removal of the brain area responsible for
seizures.
Indication: Refractory focal epilepsy.
Considerations: Pre-surgical evaluations and potential
cognitive risks.
6-Deep Brain Stimulation(DBS)
Description: Electrodes implanted in the brain
to modulate abnormal electrical activity.
Indication: Refractory epilepsy.
Considerations: Requires surgery; may not work
for all patients.
Conclusion
• - Multidisciplinaryapproach is essential for
management.
• - Need for patient-specific treatment plans.
• - Emphasis on ongoing research and patient
support systems.
32.
References
• - FisherRS, et al. Definition of drug-resistant
epilepsy: ILAE consensus.
• - Latest research articles on refractory
epilepsy.
• - Relevant clinical guidelines and textbooks.
• Uptodate
• Medical website
• CHILD NEUROLOGY AND BEYOND2023 )India
academy of pediatric)