Download to read offline
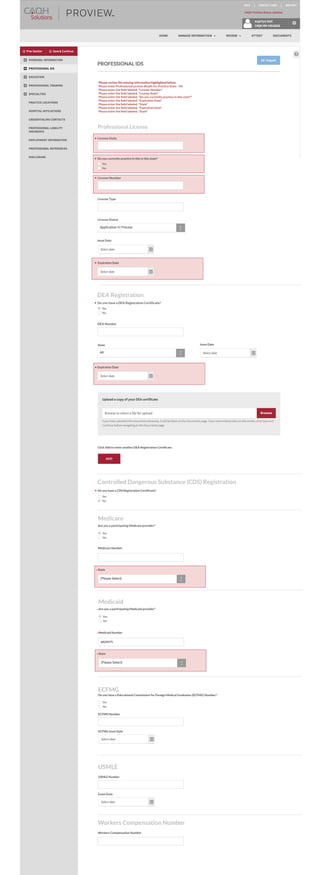





The document contains a form requesting information about a practitioner's professional licenses, certifications, and practice status. It notes several required fields need to be completed, including details about a license for the state of Virginia and expiration dates.




























