The document discusses guidelines for processing assessment data and communicating results. Key points include:
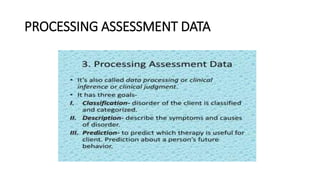
1) Assessment results should describe a client's current functioning, consider etiology factors like primary, predisposing, precipitating and reinforcing causes, and make treatment recommendations.
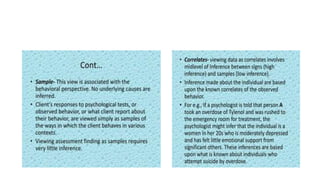
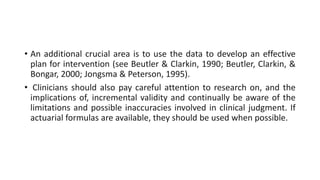
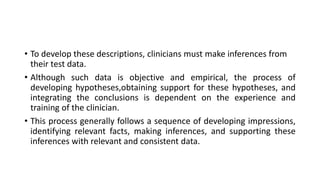
2) Clinicians should make inferences from test data to develop a deeper understanding of the client and their relationships, while being aware of limitations in clinical judgement.
3) Feedback of results should be given to clients and referral sources using clear, everyday language to effectively achieve the purpose of the assessment.



















![Psychodiagnostic technique[1]](https://cdn.slidesharecdn.com/ss_thumbnails/psychodiagnostictechnique1-191031121907-thumbnail.jpg?width=640&height=640&fit=bounds)











![Ethics[1]](https://cdn.slidesharecdn.com/ss_thumbnails/ethics1-110821092828-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)












![Introduction to applied cognitive psychology [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/introductiontoappliedcognitivepsychologyautosaved-240114110309-91a34f51-thumbnail.jpg?width=640&height=640&fit=bounds)






























