Prescribing for Heart Failure: A Guide for MBBS Students
This SlideShare presentation provides a concise reference for MBBS students on prescription writing for heart failure. It covers key medications, treatment approaches, and clinical guidelines for effective management.
Prescribing for Heart Failure: A Guide for MBBS Students
1.
Prescription Writing forHeart Failure
(HF)
A Reference Guide for MBBS Students
By Dr. Shivankan Kakkar, MD
2.
Learning Objectives
• Understandclinical features and diagnostic criteria of Heart Failure (HF)
• Learn to write accurate, safe prescriptions with precise timing for systolic and
diastolic HF
• Identify key pharmacological agents, dosages, routes, and administration
schedules
• Recognize cautions, contraindications, and monitoring needs for prescribed
drugs
• Develop skills to educate patients on medication use and disease
management
Goal: Confidently prescribe under supervision in clinical settings
3.
Introduction to HeartFailure
• Definition: Inadequate cardiac output to meet body perfusion under normal
filling pressures
• Types:
• Systolic Failure: Left ventricle loses strength, can't contract normally
(reduced ejection fraction)
• Diastolic Failure: Left ventricle can't relax, impaired filling (preserved
ejection fraction)
• Causes: Coronary artery disease, hypertensive heart disease, cardiomyopathy,
valvular disease, pulmonary vascular disease
• Stages: A (at-risk), B (structural disease, asymptomatic), C (symptomatic), D
(refractory)
4.
Salient Features ofHeart Failure
• Symptoms: Dyspnea, poor effort tolerance, peripheral edema, decreased
urine output
• Signs: Raised JVP, S3 gallop, bilateral basal crepitations, tender hepatomegaly,
ascites
• Severe Cases: Profuse pink frothy sputum (pulmonary edema), cyanosis (may
be present)
• Diagnosis:
• Chest X-ray, ECG, ABG, echocardiography
• BNP (<100 ng/L) or NT-proBNP (<300 ng/L) rules out HF
• NYHA Class (I–IV) or 6-minute walk test for severity
5.
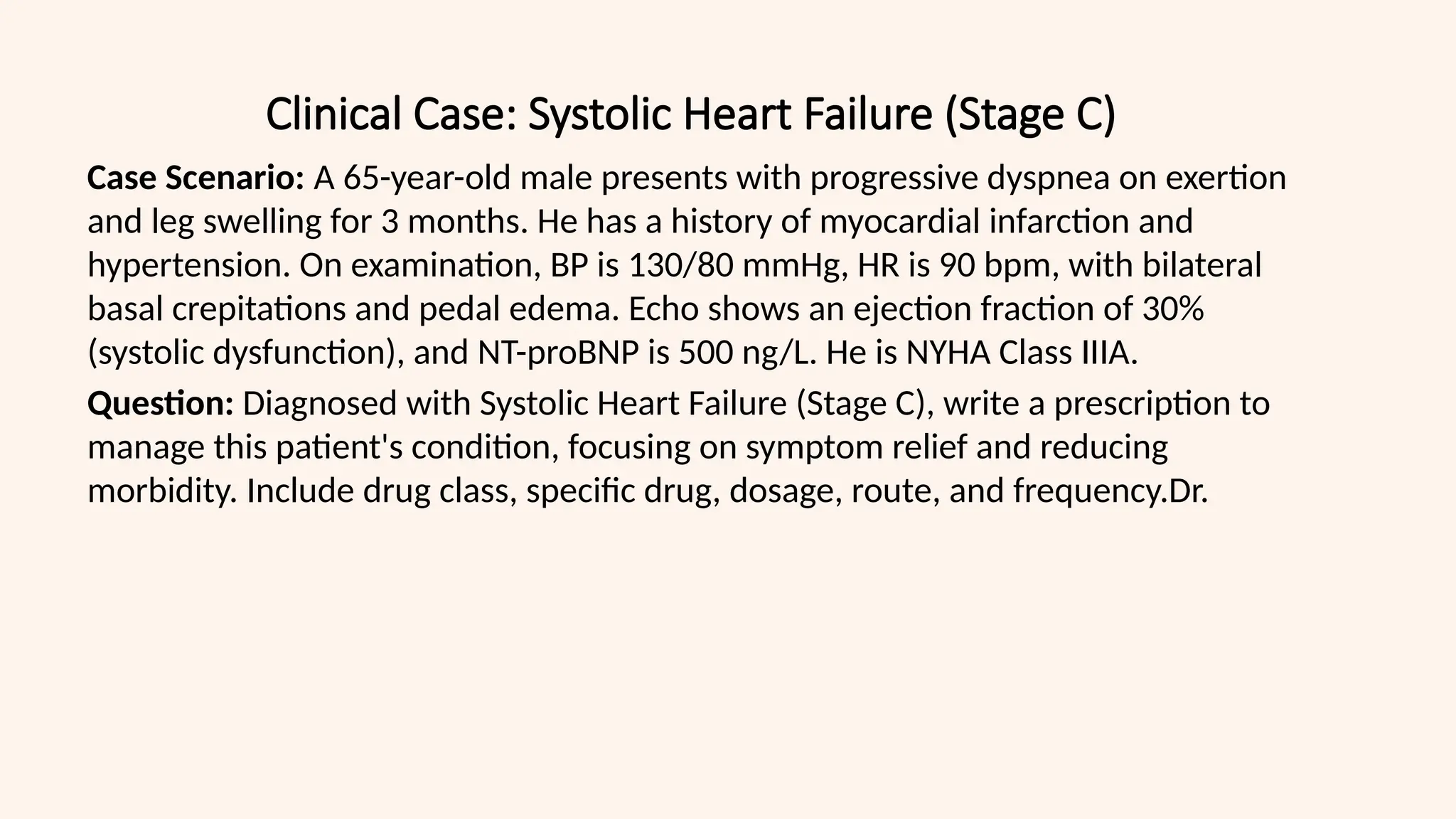
Clinical Case: SystolicHeart Failure (Stage C)
Case Scenario: A 65-year-old male presents with progressive dyspnea on exertion
and leg swelling for 3 months. He has a history of myocardial infarction and
hypertension. On examination, BP is 130/80 mmHg, HR is 90 bpm, with bilateral
basal crepitations and pedal edema. Echo shows an ejection fraction of 30%
(systolic dysfunction), and NT-proBNP is 500 ng/L. He is NYHA Class IIIA.
Question: Diagnosed with Systolic Heart Failure (Stage C), write a prescription to
manage this patient's condition, focusing on symptom relief and reducing
morbidity. Include drug class, specific drug, dosage, route, and frequency.Dr.
6.
Prescription for SystolicHeart Failure (Stage C)
Patient Name: [Name] Age/Sex: [Age/Sex] Date: [DD/MM/YYYY]
Diagnosis: Systolic Heart Failure (Stage C, NYHA IIIA)
Rx
• Tab. Torsemide 5 mg (Loop Diuretic) – Oral, BD (8 AM and 3 PM, before 4 PM
to avoid nocturia)
• Tab. Enalapril 5 mg (ACE Inhibitor) – Oral, BD (morning and evening, with
meals)
• Tab. Metoprolol-XR 25 mg (Beta-Blocker) – Oral, OD (morning, with food)
• Tab. Spironolactone 25 mg (Aldosterone Antagonist) – Oral, OD (morning,
monitor potassium)
• Tab. Atorvastatin 40 mg (Statin) – Oral, OD at bedtime (for risk factor control)
Instructions:
- Monitor electrolytes, renal function weekly initially (risk of hyperkalemia with
Spironolactone)
- Up-titrate Enalapril to 20 mg/day, Metoprolol-XR to 200 mg/day as tolerated
- Follow-up: 2 weeks, then monthly
7.
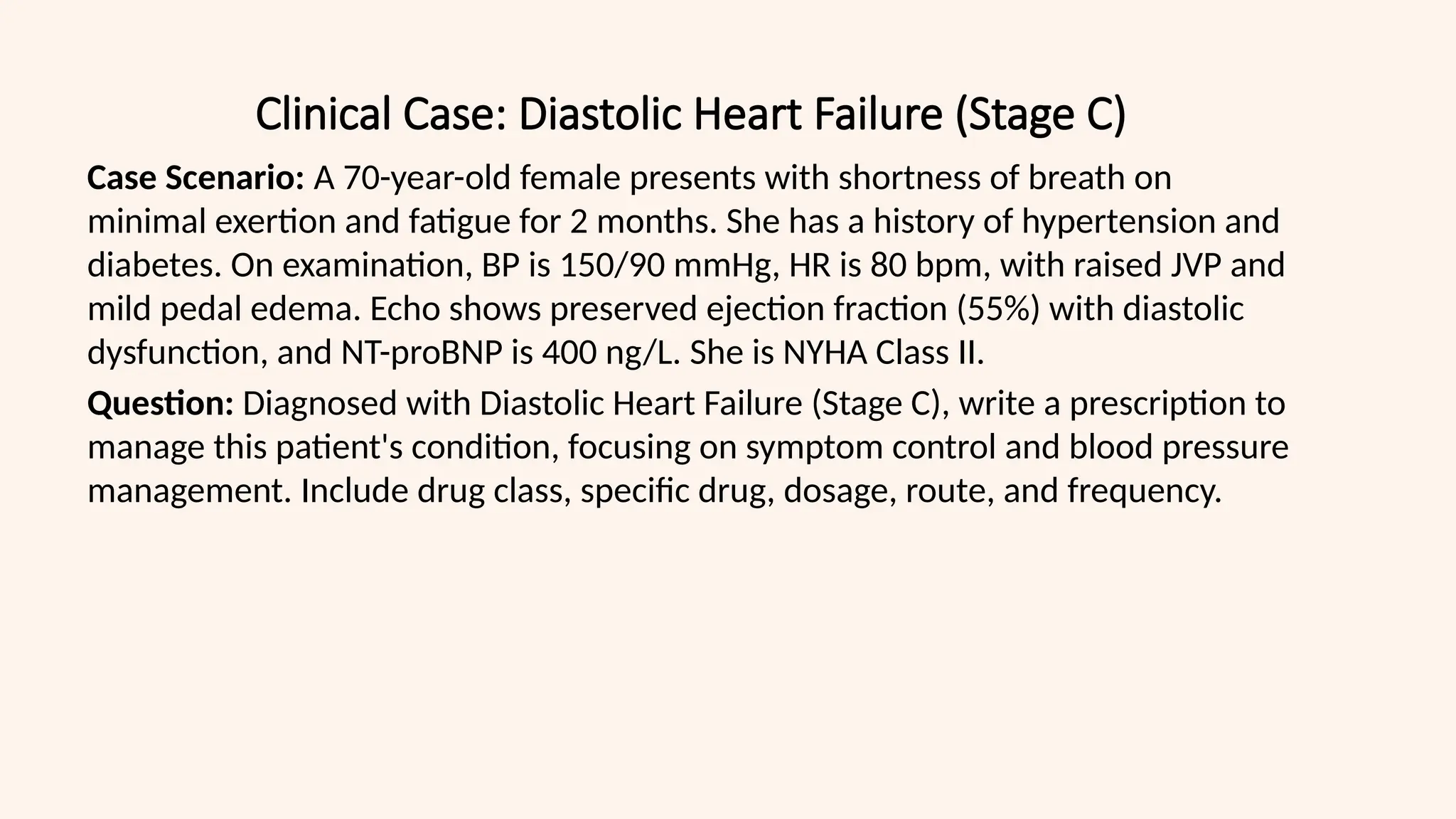
Clinical Case: DiastolicHeart Failure (Stage C)
Case Scenario: A 70-year-old female presents with shortness of breath on
minimal exertion and fatigue for 2 months. She has a history of hypertension and
diabetes. On examination, BP is 150/90 mmHg, HR is 80 bpm, with raised JVP and
mild pedal edema. Echo shows preserved ejection fraction (55%) with diastolic
dysfunction, and NT-proBNP is 400 ng/L. She is NYHA Class II.
Question: Diagnosed with Diastolic Heart Failure (Stage C), write a prescription to
manage this patient's condition, focusing on symptom control and blood pressure
management. Include drug class, specific drug, dosage, route, and frequency.
8.
Prescription for DiastolicHeart Failure (Stage C)
Patient Name: [Name] Age/Sex: [Age/Sex] Date: [DD/MM/YYYY]
Diagnosis: Diastolic Heart Failure (Stage C, NYHA II)
Rx
• Tab. Torsemide 5 mg (Loop Diuretic) – Oral, BD (8 AM and 3 PM, before 4 PM
to avoid nocturia)
• Tab. Losartan 50 mg (ARB) – Oral, OD (morning, if ACEI intolerant)
• Tab. Amlodipine 5 mg (Calcium Channel Blocker) – Oral, OD (morning, for BP
control)
• Tab. Metformin 500 mg (Antidiabetic) – Oral, BD (with meals, for diabetes
control)
• Tab. Atorvastatin 40 mg (Statin) – Oral, OD at bedtime (for risk factor control)
Instructions:
- Monitor BP (goal <130/80 mmHg), blood sugar, and renal function
- Increase Losartan to 100 mg OD if BP uncontrolled
- Follow-up: 2 weeks, then monthly
9.
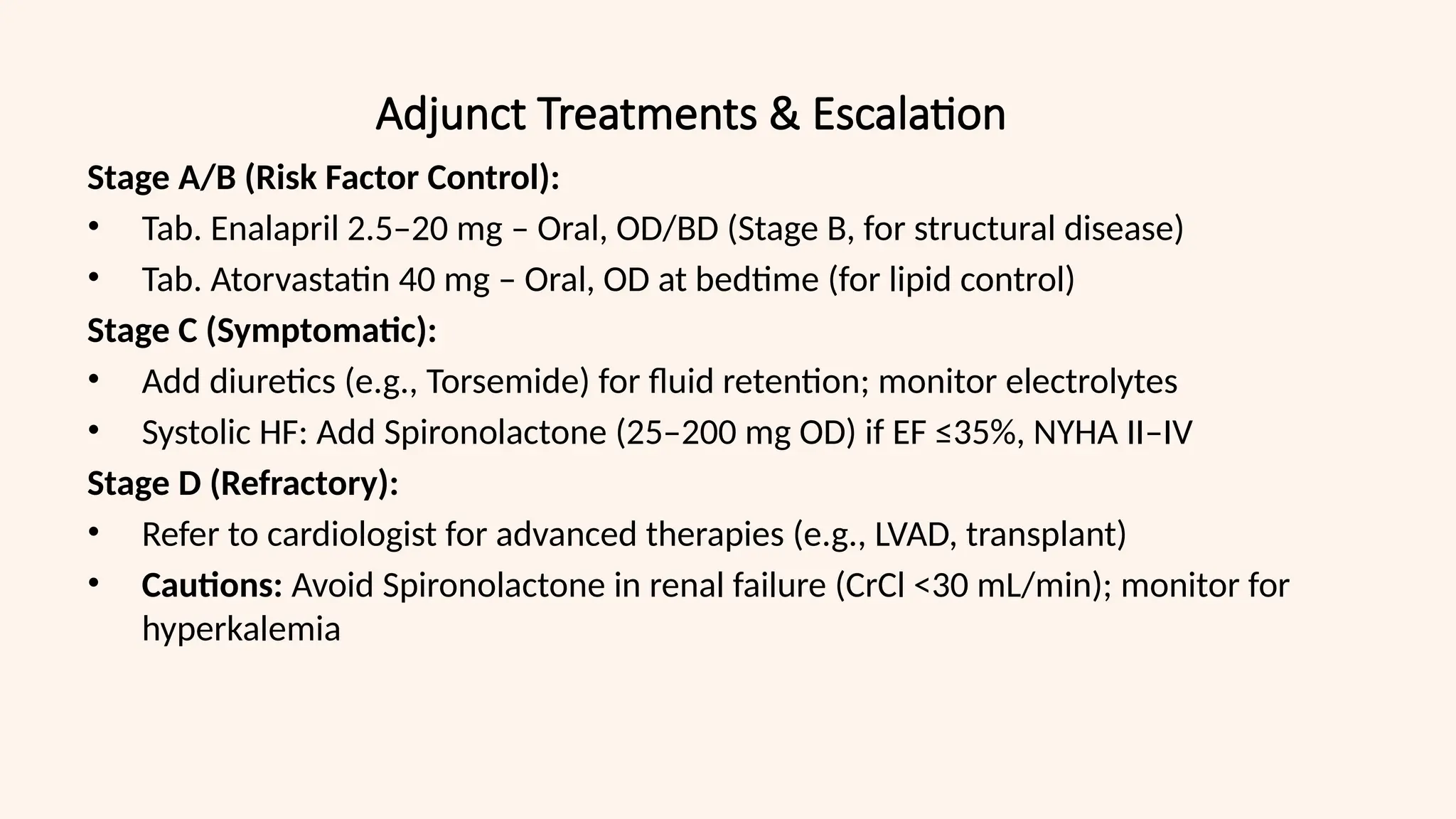
Adjunct Treatments &Escalation
Stage A/B (Risk Factor Control):
• Tab. Enalapril 2.5–20 mg – Oral, OD/BD (Stage B, for structural disease)
• Tab. Atorvastatin 40 mg – Oral, OD at bedtime (for lipid control)
Stage C (Symptomatic):
• Add diuretics (e.g., Torsemide) for fluid retention; monitor electrolytes
• Systolic HF: Add Spironolactone (25–200 mg OD) if EF ≤35%, NYHA II–IV
Stage D (Refractory):
• Refer to cardiologist for advanced therapies (e.g., LVAD, transplant)
• Cautions: Avoid Spironolactone in renal failure (CrCl <30 mL/min); monitor for
hyperkalemia
10.
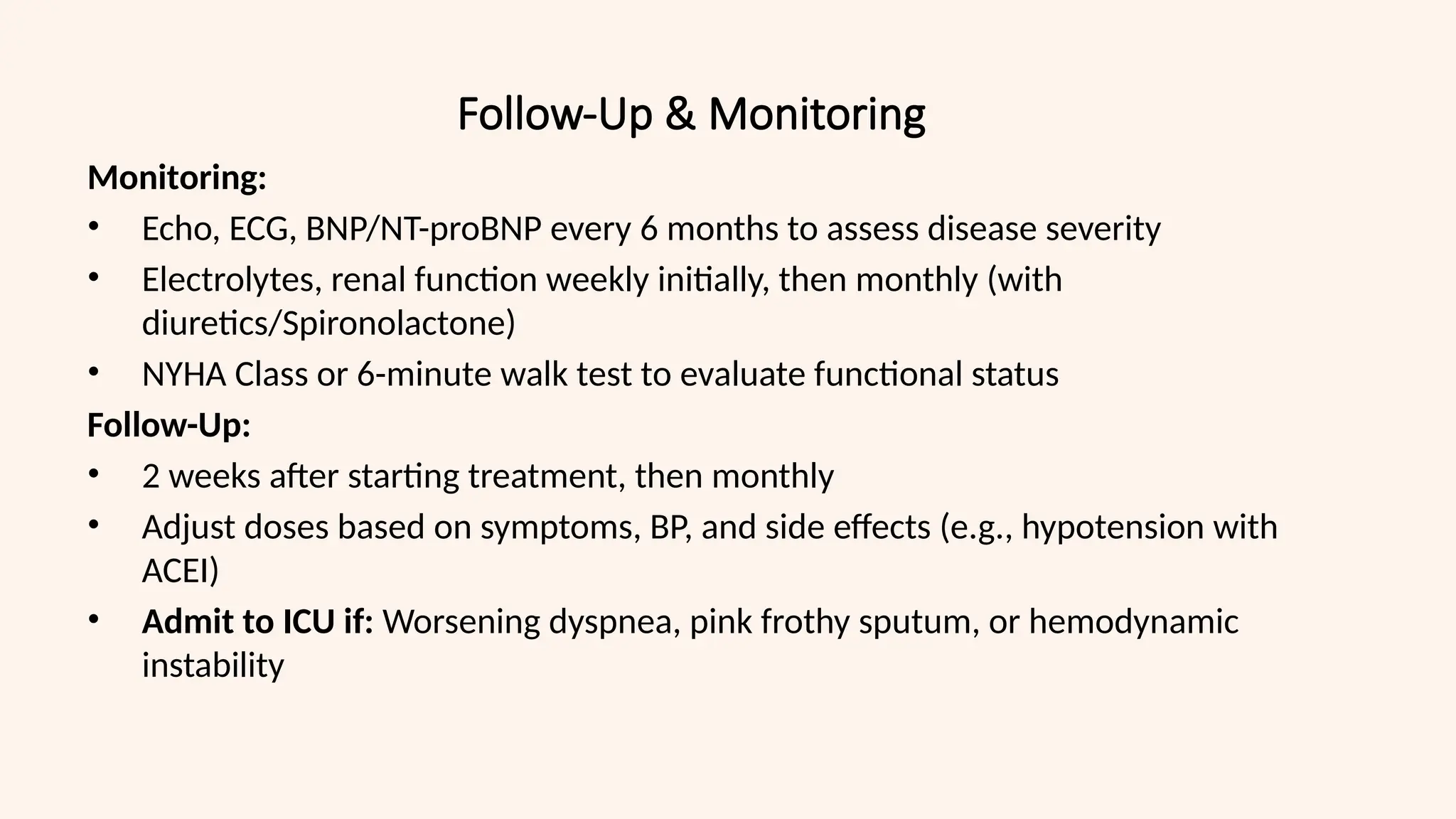
Follow-Up & Monitoring
Monitoring:
•Echo, ECG, BNP/NT-proBNP every 6 months to assess disease severity
• Electrolytes, renal function weekly initially, then monthly (with
diuretics/Spironolactone)
• NYHA Class or 6-minute walk test to evaluate functional status
Follow-Up:
• 2 weeks after starting treatment, then monthly
• Adjust doses based on symptoms, BP, and side effects (e.g., hypotension with
ACEI)
• Admit to ICU if: Worsening dyspnea, pink frothy sputum, or hemodynamic
instability
11.
Patient Education &Prevention
Key Points:
• Take Torsemide before 4 PM to avoid nighttime urination
• Lifestyle: Quit smoking, limit alcohol, reduce salt intake (<2 g/day)
• Monitor weight daily; report gain >2 kg in 3 days (fluid retention)
• Report: Worsening dyspnea, swelling, or fatigue
Prevention:
• Control risk factors: Hypertension (BP <130/80 mmHg), diabetes, lipids
• Regular follow-up to prevent progression to Stage D
12.
Drug Interactions inHeart Failure Management
• ACEIs/ARBs + Spironolactone: Risk of hyperkalemia
• Beta-blockers + Calcium Channel Blockers: Risk of heart block
• NSAIDs: Avoid in HF (fluid retention)
• Common Drug Interactions:
• Digoxin + Spironolactone: Increased digoxin levels
• Metformin + ACEIs: Monitor renal function
• Statins + Fibrates: Risk of myopathy
• Required Monitoring:
• Serum potassium
• Renal function
• Heart rate and BP
13.
Special Populations inHeart Failure
• Elderly Patients:
• Start at lower doses
• Monitor for orthostatic hypotension
• Assess cognitive function for compliance
• Renal Dysfunction:
• Adjust medication doses
• More frequent electrolyte monitoring
• Consider nephrology consultation
• Diabetes:
• Prefer ACEIs/ARBs
• Monitor glycemic control
• Consider SGLT2 inhibitors
14.
Digital Health andTelemedicine in HF
• Remote Monitoring:
• Daily weight checks
• BP monitoring
• Symptom tracking apps
• Telemedicine Follow-up:
• Virtual consultations
• Electronic prescriptions
• Digital health records
• Patient Education Resources:
• Online platforms
• Mobile apps
• Digital support groups
15.
References
References:
• Sharma S,Sethi GR. Standard Treatment Guidelines: A Manual of Medical
Therapeutics. 7th ed. New Delhi: Wolters Kluwer; 2024
• Loscalzo J, et al. Harrison's Principles of Internal Medicine. 21st ed. New York:
McGraw-Hill Education; 2024
• Indian Pharmacopoeia Commission. National Formulary of India. 6th ed.
Ghaziabad: Ministry of Health and Family Welfare; 2021
• UpToDate Inc. UpToDate: Evidence-Based Medicine. Literature review current
through Jan 2025
![Prescription for Systolic Heart Failure (Stage C)
Patient Name: [Name] Age/Sex: [Age/Sex] Date: [DD/MM/YYYY]
Diagnosis: Systolic Heart Failure (Stage C, NYHA IIIA)
Rx
• Tab. Torsemide 5 mg (Loop Diuretic) – Oral, BD (8 AM and 3 PM, before 4 PM
to avoid nocturia)
• Tab. Enalapril 5 mg (ACE Inhibitor) – Oral, BD (morning and evening, with
meals)
• Tab. Metoprolol-XR 25 mg (Beta-Blocker) – Oral, OD (morning, with food)
• Tab. Spironolactone 25 mg (Aldosterone Antagonist) – Oral, OD (morning,
monitor potassium)
• Tab. Atorvastatin 40 mg (Statin) – Oral, OD at bedtime (for risk factor control)
Instructions:
- Monitor electrolytes, renal function weekly initially (risk of hyperkalemia with
Spironolactone)
- Up-titrate Enalapril to 20 mg/day, Metoprolol-XR to 200 mg/day as tolerated
- Follow-up: 2 weeks, then monthly](https://image.slidesharecdn.com/heartfailure-250325131930-3f5d891a/75/Prescribing-for-Heart-Failure-A-Guide-for-MBBS-Students-6-2048.jpg)
![Prescription for Diastolic Heart Failure (Stage C)
Patient Name: [Name] Age/Sex: [Age/Sex] Date: [DD/MM/YYYY]
Diagnosis: Diastolic Heart Failure (Stage C, NYHA II)
Rx
• Tab. Torsemide 5 mg (Loop Diuretic) – Oral, BD (8 AM and 3 PM, before 4 PM
to avoid nocturia)
• Tab. Losartan 50 mg (ARB) – Oral, OD (morning, if ACEI intolerant)
• Tab. Amlodipine 5 mg (Calcium Channel Blocker) – Oral, OD (morning, for BP
control)
• Tab. Metformin 500 mg (Antidiabetic) – Oral, BD (with meals, for diabetes
control)
• Tab. Atorvastatin 40 mg (Statin) – Oral, OD at bedtime (for risk factor control)
Instructions:
- Monitor BP (goal <130/80 mmHg), blood sugar, and renal function
- Increase Losartan to 100 mg OD if BP uncontrolled
- Follow-up: 2 weeks, then monthly](https://image.slidesharecdn.com/heartfailure-250325131930-3f5d891a/75/Prescribing-for-Heart-Failure-A-Guide-for-MBBS-Students-8-2048.jpg)


























































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)









