CASE
The patient isa 34-year-old G3P2 (2002),
married, Filipino, Roman Catholic, from
Tatalon, Quezon City.
No known comorbidities, admitted for the
first time in the institution on December 18,
2020.
patient sought
consult atthe OPD
for prenatal check-
up
Patient denied
headache,
blurring of vision,
nausea, vomiting
1 hour PTA..
On her initial
assessment, blood
pressure was
elevated at
210/160 mmHg.
She was
immediately given
Hydralazine 5mg
IV.
HISTORY OF PRESENT ILLNESS
5.
1 hour PTA..
after15 minutes
BP was 170/100
mmHg.
Another dose of
Hydralazine 10
mg IV was given,
which lowered
the blood
pressure to
150/90 mmHg.
The patient was
subsequently
admitted.
HISTORY OF PRESENT ILLNESS
6.
OB HISTORY
Menstrual History:
●Menarche at 15, regular, every 30 days, lasting for 3 days,
soiling 2-3 moderate soaked pads per day, no
dysmenorrhea. Her last menstrual period was on April 10,
2020.
Obstetric History:
● G3P2 (2002)
● G1- 2000, live, term, female delivered by normal
spontaneous delivery, in a private hospital attended by an
OB-GYN. Diagnosed as Preeclampsia with resolution on
postpartum
● G2 - 2009, live, term, male delivered by normal
spontaneous delivery, in a private hospital attended by an
OB-GYN, 2.3kg
● G3 - Current pregnancy, with 2 prenatal consults at our
OPD
7.
OB HISTORY
Gynecologic History:
●No history of sexually transmitted infection or
abnormal vaginal discharge.
Sexual History:
● Sexual debut at the age of 23, with 1 male sexual
partner. Denies dyspareunia or post-coital bleeding.
History of Contraceptive use:
● Used injectable contraceptive last 2016 but
discontinued after 3 doses due to breakthrough
bleeding.
Immunization History:
● Received booster dose of Tetanus toxoid vaccine last
July 2020.
8.
PAST MEDICAL HISTORY
●No known co-morbidities nor allergies or trauma.
FAMILY HISTORY
SOCIAL HISTORY
● (+) Hypertension - paternal side.
● (-) Diabetes mellitus, thyroid disease, cardiac
disease, or renal disease.
● Denies smoking, alcoholic beverage drinking, or illicit
drug use.
9.
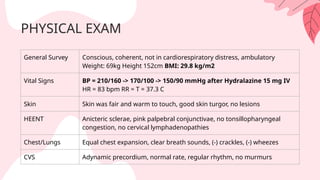
PHYSICAL EXAM
General SurveyConscious, coherent, not in cardiorespiratory distress, ambulatory
Weight: 69kg Height 152cm BMI: 29.8 kg/m2
Vital Signs BP = 210/160 -> 170/100 -> 150/90 mmHg after Hydralazine 15 mg IV
HR = 83 bpm RR = T = 37.3 C
Skin Skin was fair and warm to touch, good skin turgor, no lesions
HEENT Anicteric sclerae, pink palpebral conjunctivae, no tonsillopharyngeal
congestion, no cervical lymphadenopathies
Chest/Lungs Equal chest expansion, clear breath sounds, (-) crackles, (-) wheezes
CVS Adynamic precordium, normal rate, regular rhythm, no murmurs
10.
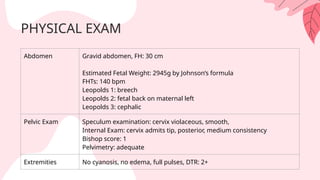
PHYSICAL EXAM
Abdomen Gravidabdomen, FH: 30 cm
Estimated Fetal Weight: 2945g by Johnson’s formula
FHTs: 140 bpm
Leopolds 1: breech
Leopolds 2: fetal back on maternal left
Leopolds 3: cephalic
Pelvic Exam Speculum examination: cervix violaceous, smooth,
Internal Exam: cervix admits tip, posterior, medium consistency
Bishop score: 1
Pelvimetry: adequate
Extremities No cyanosis, no edema, full pulses, DTR: 2+
Urinalysis 12.18.2020
Color Yellow
TurbiditySlightly hazy
Reaction Acidic
Specific Gravity 1.005
Protein Negative
Sugar Negative
RBC 0-1
WBC 0-2
Bacteria Few
Epithelial Cells Few
LABORATORIES
SALIENT POINTS
Subjective
● Identifyingdata: 34-year-old G3P2 (2002) w/ no known
comorbidities, AOG 36 weeks (DOA: Dec 18, 2020)
● 1st admission d/t chief complaint of elevated BP
● On HPI: Seen at OPD for prenatal check-up, w/ initial BP at
210/160 mmHg -> 170/100 mmHg (Hydralazine 5mg IV) ->
150/90 mmHg (Hydralazine 10mg IV)
○ No subjective complaints
○ (+) good fetal movements
15.
SALIENT POINTS
Subjective
● MenstrualHx: LMP: April 10, 2020
● Obstetric Hx: history of preeclampsia w/ resolution on
postpartum (G1), currently on 3rd pregnancy w/ 2
prenatal consults at OPD
● Contraceptive Hx: Discontinued use of injectable
contraceptive use (2016) after 3 doses d/t
breakthrough bleeding
● Family Hx: HTN on paternal side
16.
SALIENT POINTS
OBJECTIVE
● BMIof 29.8 = Obese
● Hypertensive: BP initially at 210/120 decreased to
→
150/90 after a total of Hydralazine 15mg IV
● Lab findings:
○ Physiologic elevation of WBC and urine protein
creatinine ratio
○ Normal findings: negative protein on urine, LDH,
SGPT/ SGOT, platelets, creatinine
17.
ADMITTING DIAGNOSIS
G3P2 (2002)Pregnancy Uterine 36 weeks
AOG by LMP, cephalic not in labor;
Preeclampsia with Severe Features
18.
PLAN
Admit for BPcontrol, seizure prophylaxis,
late preterm steroid administration,
induction of labor
19.
Patient was given:
●Magnesiumsulfate 4g
loading dose by slow IV
push
●Magnesium sulfate drip:
D5W 500cc + 20g MgSO4
ran at 1g/hour.
●1st dose of Dexamethasone
6mg IM
Day of Admission
●BP controlled at 150/90 mmHg
after Hydralazine 15 mg IV
●Preeclampsia work-up was
normal.
●Given Methyldopa 250mg/tab,
2tab Q4
●Negative contraction stress test
●Cervical priming done using
Dinoprostone gel (Primigyn)
● While on continuous
Mg sulfate drip, serum
Mg elevated to 7.5
mEq/L -> placed on hold
for possible Mg toxicity.
Course in the Ward
On 8th hour
20.
●BP range at140-150/ 90-
100 mmHg, no subjective
complaints.
●Non-stress test reactive,
hooked to fetal monitor.
1st hospital day
●IE: 1cm dilated cervix, 50%
effacement, cephalic, station -3,
intact membranes, medium in
consistency, posterior in
location, Bishop Score of 2. 2nd
dose Dinoprostone gel
(Primigyn) given & Mg sulfate
drip resumed
● cervical reassessment had same
findings. 3rd dose of Dinoprostone
(Primigyn) given. After completing
3 doses of Dinoprostone for 24
hours, w/ same IE findings,
induction of labor was done, px
given oxytocin.
Course in the Ward
After 8 hours
After 8 hours
21.
●emergency primary lowsegment
CS done for non-reassuring FHR
pattern with persistent variable
decelerations/ pathologic feature
1st hospital day, after 4hrs of
induction of labor
●Intraoperatively, head was at right occiput transverse,
with 1 loose loop of nuchal cord, amniotic fluid was
thinly stained and scanty, placenta at the antero-
fundal area, with an estimated blood loss of 300cc. The
placenta was grossly normal and was sent for
histopathologic report.
Course in the Ward
22.
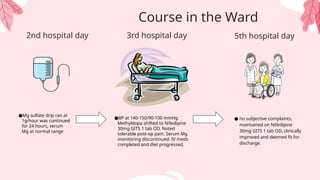
●Mg sulfate dripran at
1g/hour was continued
for 24 hours, serum
Mg at normal range
2nd hospital day
●BP at 140-150/90-100 mmHg.
Methyldopa shifted to Nifedipine
30mg GITS 1 tab OD. Noted
tolerable post-op pain. Serum Mg
monitoring discontinued. IV meds
completed and diet progressed.
● no subjective complaints,
maintained on Nifedipine
30mg GITS 1 tab OD, clinically
improved and deemed fit for
discharge.
Course in the Ward
5th hospital day
3rd hospital day
23.
DISCHARGE DIAGNOSIS
G3P3 (2103)Pregnancy Uterine
delivered live preterm, cephalic, male,
BW 2100g, AGA, BL 45cm AS 9&9,
Ballard Score 36 weeks by Emergency
Primary Low Segment Cesarean
Section under Spinal Anesthesia;
Preeclampsia with Severe Features
● Preeclampsia occursin..
○ 5% to 6% of live births
○ Most common - third trimester near term
○ 80% develop HELLP syndrome after preeclampsia
diagnosis (30% without severe features, 50% with severe
features)
● According to WHO Maternal Mortality 2017
○ Severe Bleeding (mostly bleeding after childbirth)
○ Infections (usually after childbirth)
○ High blood pressure during pregnancy (pre-
eclampsia and eclampsia)
■ Considered number 1 cause in the Philippines (DOH
Epid Bureau, 2017)
27.
RISK FACTORS
○ Young
○Nulliparous
○ Obesity
○ Diabetes
○ Chronic Hypertension
○ Prior Preeclampsia (highest risk)
○ Family history of preeclampsia
○ Advanced maternal age
○ Autoimmune disorders (collagen vascular disease)
○ Short inter-pregnancy interval
○ Hydrops Fetalis
○ Molar pregnancy
○ Race ethnicity (higher in African Americans)
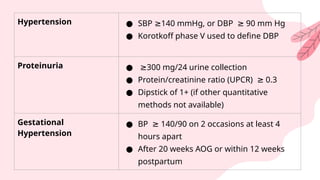
Hypertension ● SBP140 mmHg, or DBP 90 mm Hg
≥ ≥
● Korotkoff phase V used to define DBP
Proteinuria ● ≥300 mg/24 urine collection
● Protein/creatinine ratio (UPCR) 0.3
≥
● Dipstick of 1+ (if other quantitative
methods not available)
Gestational
Hypertension
● BP 140/90 on 2 occasions at least 4
≥
hours apart
● After 20 weeks AOG or within 12 weeks
postpartum
30.
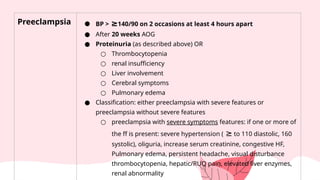
Preeclampsia ● BP> ≥140/90 on 2 occasions at least 4 hours apart
● After 20 weeks AOG
● Proteinuria (as described above) OR
○ Thrombocytopenia
○ renal insufficiency
○ Liver involvement
○ Cerebral symptoms
○ Pulmonary edema
● Classification: either preeclampsia with severe features or
preeclampsia without severe features
○ preeclampsia with severe symptoms features: if one or more of
the ff is present: severe hypertension ( ≥ to 110 diastolic, 160
systolic), oliguria, increase serum creatinine, congestive HF,
Pulmonary edema, persistent headache, visual disturbance
thrombocytopenia, hepatic/RUQ pain, elevated liver enzymes,
renal abnormality
31.
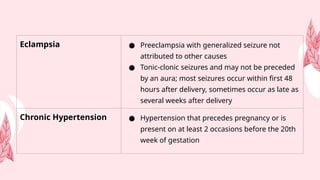
Eclampsia ● Preeclampsiawith generalized seizure not
attributed to other causes
● Tonic-clonic seizures and may not be preceded
by an aura; most seizures occur within first 48
hours after delivery, sometimes occur as late as
several weeks after delivery
Chronic Hypertension ● Hypertension that precedes pregnancy or is
present on at least 2 occasions before the 20th
week of gestation
32.
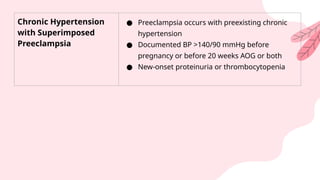
Chronic Hypertension
with Superimposed
Preeclampsia
●Preeclampsia occurs with preexisting chronic
hypertension
● Documented BP >140/90 mmHg before
pregnancy or before 20 weeks AOG or both
● New-onset proteinuria or thrombocytopenia
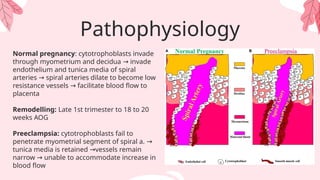
Pathophysiology
Normal pregnancy: cytotrophoblastsinvade
through myometrium and decidua invade
→
endothelium and tunica media of spiral
arteries spiral arteries dilate to become low
→
resistance vessels facilitate blood flow to
→
placenta
Remodelling: Late 1st trimester to 18 to 20
weeks AOG
Preeclampsia: cytotrophoblasts fail to
penetrate myometrial segment of spiral a. →
tunica media is retained vessels remain
→
narrow unable to accommodate increase in
→
blood flow
Pathophysiology
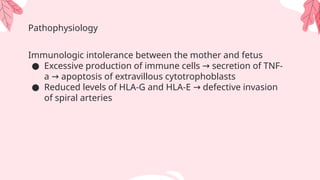
Immunologic intolerance betweenthe mother and fetus
● Excessive production of immune cells secretion of TNF-
→
a apoptosis of extravillous cytotrophoblasts
→
● Reduced levels of HLA-G and HLA-E defective invasion
→
of spiral arteries
39.
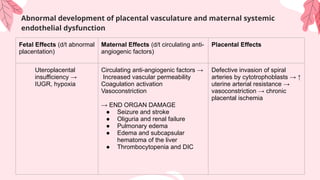
Abnormal development ofplacental vasculature and maternal systemic
endothelial dysfunction
Fetal Effects (d/t abnormal
placentation)
Maternal Effects (d/t circulating anti-
angiogenic factors)
Placental Effects
Uteroplacental
insufficiency →
IUGR, hypoxia
Circulating anti-angiogenic factors →
Increased vascular permeability
Coagulation activation
Vasoconstriction
→ END ORGAN DAMAGE
● Seizure and stroke
● Oliguria and renal failure
● Pulmonary edema
● Edema and subcapsular
hematoma of the liver
● Thrombocytopenia and DIC
Defective invasion of spiral
arteries by cytotrophoblasts → ↑
uterine arterial resistance →
vasoconstriction → chronic
placental ischemia
40.
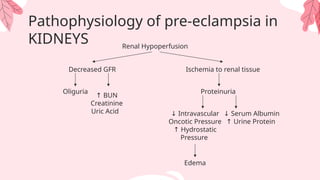
Pathophysiology of pre-eclampsiain
KIDNEYS Renal Hypoperfusion
Decreased GFR Ischemia to renal tissue
Oliguria Proteinuria
↓ Intravascular
Oncotic Pressure
↑ Hydrostatic
Pressure
↓ Serum Albumin
↑ Urine Protein
Edema
↑ BUN
Creatinine
Uric Acid
41.
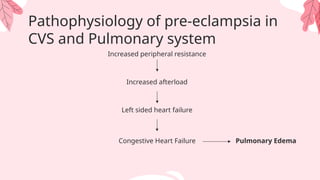
Pathophysiology of pre-eclampsiain
CVS and Pulmonary system
Increased peripheral resistance
Increased afterload
Left sided heart failure
Congestive Heart Failure Pulmonary Edema
42.
Pathophysiology of pre-eclampsiain
Gastrointestinal
Liver ischemia
Liver cell necrosis
Release of liver enzymes (SGPT/ALT) into
the blood
Liver edema and Hydropic degeneration of the
liver cells
Stretching of glisson’s capsule
Epigastric or RUQ pain
43.
Pathophysiology of pre-eclampsiain
CNS
CNS
Meningeal
irritation
Headache
Retinal
ischemia
Neuronal
ischemia/irritation
CVA
Blurring
of vision
Convulsions
● Blood pressuremeasurement
○ Routinely used as screening tool
○ Obtained during each prenatal care
○ Diagnosis: >/= 140/90 mmHg on 2 occasions 4 hrs apart, after 20 wks
or proteinuria or in absence of proteinuria, thrombocytopenia, renal
insufficiency, impaired liver function, pulmonary edema, or cerebral or
visual symptoms
● Uterine artery doppler
○ Done to estimate resistance to uteroplacental blood flow
○ Faulty trophoblastic invasion of the spiral arteries results in diminished
placental perfusion and increased uterine artery resistance
○ Increased flow resistance results in an abnormal waveform
represented by an exaggerated diastolic notch
Screening for preeclampsia
46.
● Roll OverTest
○ Can be done in the outpatient or in primary care setting
○ Measures the hypertensive response in women at 28 to 32 weeks who are
resting in the left lateral decubitus position and then roll over to the supine
position
○ The roll-over test is considered positive if the diastolic blood pressure
increased 20 mmHg or more in supine, with respect to that obtained in
lateral decubitus, at 1 and at 5 minutes.
● SFIt-1 and PIGF
○ SFlt-1 levels begin to increase in maternal serum months before
preeclampsia while high levels in the second trimester were associated with
a doubling of the risk for preeclampsia
Screening for preeclampsia
47.
● Accurate assessmentof blood pressure
● CBC - to check for anemia & thrombocytopenia
● 12 L ECG - to check for presence of chamber enlargement
● Blood chemistry - to check for secondary causes of
hypertension and comorbidities such as DM; end-organ
damage, presence of features of severe pre-eclampsia
● TSH - to evaluate for secondary causes of hypertension
● LDH - to assess hemolysis in possible HELLP syndrome
General Work-up
48.
● Liver enzymes(AST, ALT)
● 24 H urine collection; Protein-to-creatinine ratio
● Fetal monitoring (BPP or NST); ultrasound (evaluate amniotic
fluid volume and estimate fetal weight)
● EEG - to evaluate patients presenting with neurologic
deficits/severe persistent headache
Evaluation of pre-eclampsia/eclampsia
Preventive Management
● Lowdose aspirin
○ For those with 2 moderate risk factors
≥
■ Nulliparity
■ Obesity
■ Family history of preeclampsia
■ Age 35 years
≥
■ Sociodemograpahic factors
■ Personal risk factors
■ In-vitro conception
○ 60-150 mg/day at night starting at 11-14 weeks gestation or <16 weeks
until 36 weeks AOG
● Calcium supplementation
○ recommended 1500-2000 mg elemental calcium supplementation per day
● Exercise
● Antioxidants
51.
Definitive Treatment
Preeclampsia of37 weeks or later
● Fetus delivery to treat preeclampsia and prevent complication
Preeclampsia on less than 37 weeks
● Mild Preeclampsia: may continue pregnancy with close monitoring of
the fetus
○ Continue pregnancy until 37 weeks for delivery
○ Anti-hypertensive medication
○ Weekly laboratory test
● Severe Preeclampsia: admission to the hospital for close and continuous
monitoring
○ Fluid management, seizure prevention, lowering BP
○ Pregnancy of 34 weeks or later: delivery as soon as possible
○ Pregnancy or less than 34 weeks: betamethasone or
dexamethasone
52.
Definitive Treatment
Indications forDelivery in Pre-eclampsia Regardless of AOG
Maternal Indications Fetal Indication
● Eclampsia
● Recurrent symptoms of severe
preeclampsia
● Uncontrollable severe HPN
● Progressive renal insufficiency
● Persistent thrombocytopenia or
HELLP syndrome
● Pulmonary edema
● Suspected abruptio placenta
● Progressive labor or rupture of
● Severe Fetal growth restriction
● Persistent oligohydramnios
● Abnormal fetal surveillance tests
(BPP, umbilical artery doppler
studies, decelerations on NST)
● Fetal death in utero
53.
Definitive Treatment
Control ofconvulsions
● Seizure prophylaxis is not required unless severe features develop
● Severe headache, visual disturbances, and hyperreflexia may signal
impending eclamptic seizure
● Anticonvulsive medication, such as magnesium sulfate, might be
used to prevent a seizure in women who have preeclampsia with
severe features.
54.
Intrapartum Management
● Ripeningagents & induction of labor may be used
● Factors such as prolonged induction, nulliparity, <32 weeks of
gestation, unfavorable cervix & non-reassuring fetal status may
warrant cesarean delivery
● Hypertension - Hydralazine / Labetalol / Methyldopa
● Fluid management: maintenance of NSS at around 80cc/hr
● Seizure prophylaxis: MgSO4
○ Loading dose: 4-6g of 10% solution IV over 20mins
○ Continuous infusion: 1-2g / hr
○ Contraindication: myasthenia gravis, levetiracetam may be
used
● Platelet transfusion must be readied for <50,000 microL
55.
Management of MildPreeclampsia
● General medical
○ 1st line management: methyldopa 500 mg every 6-8 hours
○ 2nd line drug: hydralazine 25 mg every 6-12 hours
○ MgSO4 for seizure protection
○ Aspirin
● Timing of delivery and management
○ Term pregnancies deliver
→
○ Preterm pregnancy expectant management
→
■ Close monitoring
● Fetal well being
● Blood pressure monitoring and treatment
● includes lab follow up for platelet count, serum crea, serum
aminotransferase
■ Patient education and counseling of the signs and symptoms of the severe
disease spectrum, fetal movements
■ Restricted activity recommended, strict bedrest unnecessary, lateral decubitus
position advised when lying down
■ Antenatal corticosteroids if birth within 7 days is expected
56.
Management of ChronicHypertension
● Utilize BP 140/90 as threshold for initiation/titration of medical
therapy (vs. previous threshold BP 160/110) (ACOG, 2022)
● Anti-HPN medications safe during pregnancy:
○ Methyldopa: 2-3x daily up to 3,000 mg per day
○ Labetalol: 2x daily up to 2,400 mg/day in women w/o
asthma, myocardial disease, dec. cardiac function, heart
block, bradycardia
○ Extended-release nifedipine: up to 120 mg daily in women
w/o tachycardia
○ Hydrochlorothiazide, 12.5-25 mg daily
● Avoid use of ACEi, ARBs, renin inhibitors, mineralocorticoid
receptor antagonists
57.
Management of ChronicHypertension
● Obtain baseline laboratory work-ups such as:
○ CBC
○ Complete metabolic panel
○ Baseline 24-hour urine for creatinine clearance and protein
○ Baseline ECG
● Initial low-dose aspirin after 12 weeks
○ Reduce risk of superimposed preeclampsia
58.
August, P., &Sibai, B. (2023). Preeclampsia: Clinical features and diagnosis. UpToDate. Retrieved January 22, 2023 from
https://www.uptodate.com/contents/preeclampsia-clinical-features-and-diagnosis?
search=preeclampsia&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1#H3583231095
American College of Obstetricians and Gynecologists (2020). Gestational Hypertension and Preeclampsia. Obstetrics &
Gynecology, 135(6), e237–e260. doi:10.1097/aog.0000000000003891
Croke L. (2019). Managing Chronic Hypertension in Pregnant Women: ACOG Releases Updated Practice Bulletin. American
family physician, 100(12), 782–783.
Cunningham, F. G., Leveno, K. J., Dashe, J. S., Hoffman, B. L., Spong, C. Y., & Casey, B. M. (Eds.). (2022). Williams Obstetrics
(26th ed.). McGraw-Hill Education.
Karumanchi, S., Lim, K., & August, P. (2022). Preeclampsia: pathogenesis. UpToDate. Retrieved January 22, 2022, from
https://www.uptodate.com/contents/preeclampsia-pathogenesis?
search=preeclampsia&source=search_result&selectedTitle=5~150&usage_type=default&display_rank=5#H3
Norwitz, E. (2022). Preeclampsia: Antepartum management and timing of delivery. Uptodate. Retrieved January 19, 2022, from
https://www.uptodate.com/contents/preeclampsia-antepartum-management-and-timing-of-delivery?
search=preeclampsia&source=search_result&selectedTitle=2~150&usage_type=default&display_rank=2#H5
Uzan, J., Carbonnel, M., Piconne, O., Asmar, R., Ayoubi, J.M. (2011). Pre-eclampsia: pathophysiology, diagnosis, and
management. Vasc Health Risk Manag. 2011;7:467-74. doi: 10.2147/VHRM.S20181. Epub 2011 Jul 19. PMID: 21822394;
PMCID: PMC3148420
References
#1 Good am! We’re Team 4, varela-zantua, from group 7B, and our case conference for today is about preeclampsia
We’ll start by presenting our case then we’ll proceed with the discussion of preeclampsia
#2 This is a case of a 34-year-old G3P2 (2002), married, Filipino, Roman Catholic, from Tatalon, Quezon City, with no known comorbidities, admitted for the first time in the institution on December 18, 2020.
#3 The patient came in with chief complaint of Elevated Blood pressure
#5 One hour prior to admission, the patient sought consult at the out-patient department for prenatal check-up. The patient had no subjective complaints such as headache, blurring of vision, nausea, vomiting.
On her initial assessment, blood pressure was elevated at 210/160 mmHg. The patient was immediately given Hydralazine 5mg IV.
The blood pressure after 15 minutes was 170/100 mmHg. Another dose of Hydralazine 10 mg IV was given, which lowered the blood pressure to 150/90 mmHg. The patient was subsequently admitted.
Pertinent Positives & Negatives
(-) Headache, difficulty of breathing, epigastric pain
(-) Watery vaginal discharge, vaginal bleeding
(+) good fetal movements
MAP= DP + 1/3(SP – DP)
BP 210/160
MAP = 176.67
BP 170/100
MAP = 123.33
BP 150/90
MAP = 110
MAP >90: increased risk??
Hydralazine: direct acting vasodilator, when given as a rescue dose: 5 mg IV PRN q 20 mins for BP >/= 160/100 (max 30 mg, 5-5-5-10-10)
#6 The blood pressure after 15 minutes was 170/100 mmHg. Another dose of Hydralazine 10 mg IV was given, which lowered the blood pressure to 150/90 mmHg. The patient was subsequently admitted.
Pertinent Positives & Negatives
(-) Headache, difficulty of breathing, epigastric pain
(-) Watery vaginal discharge, vaginal bleeding
(+) good fetal movements
MAP= DP + 1/3(SP – DP)
BP 210/160
MAP = 176.67
BP 170/100
MAP = 123.33
BP 150/90
MAP = 110
#9
Family history of hypertension or cardiovascular disease is associated with a higher risk of developing preeclampsia
#10 BMI: 29.8 kg/m2 (Obese I, WHO “Asian Criteria” values) which may contribute as a maternal risk factor highly associated with preeclampsia.
MAP= DP + 1/3(SP – DP)
BP 210/160
MAP = 176.67
BP 170/100
MAP = 123.33
BP 150/90
MAP = 110
#11 Fetal Weight in grams = 155 x (Fundal Height in cm - K)
○ K = 11 (fetal head at plus station)
○ K = 12 (fetal head at zero station)
○ K = 13 (fetal head at minus station)
n = 12: if head is unengaged (- station); 11: if head is
engaged (+ station)
= 155 x (30-11) = 2945g (pero mali to, dapat 30 minus 13 kasi minus station pa siya eh so 2790 dapat); EFW appropriate for gestational age. By week 36 of pregnancy fetal weight is approximately 2.7kg and fetal length is around 47.5cm from crown to heel.
L1: What occupies the uterine fundus?
○ L2: Where is the fetal back, small parts, FHT?
○ L3: What is the presenting part? Engagement?
L4: Where is the cephalic prominence?
■ Is the head extended or flexed?
Bishop score 1: Dilation 1-2 cm, Effacement 40-50%, Station -2, Consistency medium, Position midposition; As the patient is not yet in labor, the low Bishop score of < 4: unfavorable cervix and may be an indication for cervical ripening.
#12 CBC - normal hgb, hct, but slightly elevated wbc count (normal range: 5.0-10.0 x10^9/L), although normal physiologic increase in pregnancy; Typically, white blood cell count is elevated during pregnancy, with the lower limit of the reference range being around 6,000 cells per μl and the upper limit around 15,000 cells per μl. May reach 25,000 if during labor. Leucocytosis, occurring during pregnancy is due to the physiologic stress induced by the pregnant state
Biochemistry - elevated upcr (Normal range <20mg/mmol)
Indicates abnormal levels of urine protein or albumin; However, the american college of obstetricians and gynecologists recommends a P/C ratio of 30 mg/mmol (0.3 mg/mg) for the classification of proteinuria in pregnant women at risk of preeclampsia. Thus a slightly elevated upcr in our patient’s case might merit consideration of trace proteinuria, but does not reach the cut-off value for pathologic proteinuria in pregnancy.
Patient has a normal platelet count 150-440,000
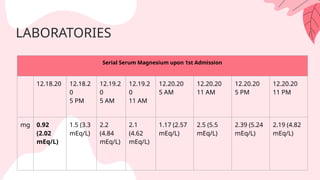
#14 Previous studies have shown a significant reduction in the level of serum magnesium in pregnant mothers with pre-eclampsia (7). This result agrees with the physiological role of magnesium; magnesium is one of the essential intracellular cations and an important cofactor for activation of many enzymes. Magnesium has a significant role in pathophysiological regulation of blood pressure because it affects contractility and tone of blood vessels. The decrease of serum Mg we see here is consistent with the increased blood pressure of the patient.
Normal range: 1.3 to 2.1 mEq/L
#15 Ok, thank you __, to review the salient points of the case
We have a 34-year-old G3P2 (2002) w/ no known comorbidities, AOG 36 weeks which is on late preterm (DOA: Dec 18, 2020)
This is her 1st admission d/t cc of elevated BP which was initially at 210/160. However it decreased to 150/90 after a total of 15mg Hydralazine IV, with good fetal movements
#16
Last menstrual period was Apr 10, 2020 with obstetric history of preeclampsia w/ resolution on 1st pregnancy. She is currently on her 3rd pregnancy w/ 2 prenatal consults at the OPD. Px had contraceptive hx of discontinuation of use of injectable contraceptives last 206 after 3 doses d/t breakthrough bleeding and a family hx of htn on paternal side
#17 On PE patient’s BMI showed 29.8 which is classified as obese, hypertensive, abdominal and pelvic exam showed patient is not in labor, and a physiologic elevation of WBC and urine protein creatinine ratio on lab findings.
Asian-Pacific (BMI)
Obese I: 25.0 - 29.9
Although leukocyte count are usually higher than nonpregnant values since this is associated with physiologic stress induced by the pregnant state
** leukocyte count are usually higher than nonpregnant values, and the upper values approach 15,000/μL. During labor and the early puerperium, values may become markedly elevated, attaining levels of 25,000/μL which may be associated with physiologic stress induced by the pregnant state
#20 A short discussion on what happened to her during her admission, on the day of admission patient was given seizure prophylaxis in the form of Magnesium sulfate 4g loading dose by slow IV push followed by Magnesium sulfate drip. First dose of Dexamethasone 6mg IM was administered for late preterm antenatal corticosteroids.
Blood pressure was controlled at 150/90 mmHg after a total of Hydralazine 15 mg IV. Complete preeclampsia work-up revealed normal results. The patient was given Methyldopa 250mg/tab, 2 tablets given every 6 hours. She ahd negative contraction stress test and ervical priming done using Dinoprostone gel (Primigyn).
However on the 8th hour while being on continuous magnesium sulfate drip, serum magnesium was noted to be elevated to 7.5 mEq/L. This was then put on hold and patient was observed for symptoms of magnesium toxicity
#21 On the 1st hospital day, blood pressure ranged from 140-150/90-100 mmHg, non-stress test was reactive and patient was hooked to fetal monitor.
After 8 hours, internal examination revealed a 1cm dilated cervix, with 50% effacement, cephalic, station -3, intact membranes, medium in consistency, and posterior in location, with Bishop Score of 2. Second dose of Dinoprostone gel (Primigyn) was given. Magnesium sulfate drip was resumed for seizure prophylaxis.
After another eight hours, cervical reassessment had the same findings. Third dose of Dinoprostone (Primigyn) was given. After completing three doses of Dinoprostone for 24 hours, with the same internal examination findings, induction of labor was continued using oxytocin
#22 After 4 hours of induction of labor, an emergency primary low segment cesarean section was called for non-reassuring fetal heart rate pattern with persistent variable decelerations with pathologic features. Intraoperatively, the head was at right occiput transverse, with 1 loose loop of nuchal cord, amniotic fluid was thinly stained and scanty, placenta at the antero-fundal area, with an estimated blood loss of 300cc. The placenta was grossly normal and was sent for
histopathologic report.
#23 On second hospital day, Magnesium sulfate drip ran at 1g/hour was continued for 24 hours. Serial serum magnesium monitoring every 6 hours were all within therapeutic range.
On the 3rd hospital day, blood pressure ranged at 140-150/90-100 mmHg. Methyldopa was shifted to Nifedipine 30mg GITS gastrointestinal therapeutic system 1 tablet once daily. No subjective complaints from the patient however there was minimal but tolerable post-operative pain. Serial serum magnesium monitoring was discontinued. IV medications were completed and diet was progressed accordingly.
On the 5th hospital stay, patient had no subjective complaints with BP ranged at 130- 140/80-90 mmHg, she was maintained on Nifedipine 30mg GITS 1 tablet once daily. On inspection, with well coaptated wound, no abnormal discharge. Patient’s condition clinically improved and was deemed fit for discharge.
#25 For the discussion of pre eclampsia, we will be following this order
#27 Preeclampsia occurs in..
5% to 6% of live births
Most common - third trimester near term
80% develop HELLP syndrome after preeclampsia diagnosis
According to WHO, these are the top three causes of maternal mortality last 2017
Severe Bleeding (mostly bleeding after childbirth)
Infections (usually after childbirth)
High blood pressure during pregnancy (pre-eclampsia and eclampsia)
However in the Philippines, the main cause of maternal mortality is usually pre eclampsia and gestational hypertension
#28 Risk factors of preeclampsia include
Those who are young
Nulliparous women, though it is unclear why nulliparity is consistently found to be one of the predisposing factor for preeclampsia, one theory suggests that the immune system of nulliparous women has had limited exposure to paternal antigens which plays a role in the pathogenesis of preeclampsia that will be discuss later
Obesity, The risk of preeclampsia in obese individuals doubles with each 5 to 7 kg/m2 increase in prepregnancy body mass index
Those who have pre-existing medical conditions like Diabetes and chronic hypertension, This increase has been related to a variety of factors, such as underlying renal or vascular disease, obesity, high plasma insulin levels/insulin resistance, and abnormal lipid metabolism
A prior history of pre eclampsia increases the risk of developing preeclampsia in a subsequent pregnancy, as weel as a family history of preeclampsia
Advanced maternal age because Older patients tend to have additional risk factors, such as obesity, diabetes mellitus, and chronic hypertension, that predispose them to developing preeclampsia.
Autoimmune disorders like SLE. the reasons for this relationship are not clear but may include multiple mechanisms involving inflammation, microangiopathy, increased platelet turnover, and kidney dysfunction.
Other risk factors include Short inter-pregnancy interval, Hydrops Fetalis, Molar pregnancy, And some Minority racial groups , it is said to be higher in african americans
As for our case, obesity and a previous history of pre eclampsia on her first pregnancy are the risk factors present for our patient
#29 In this part, we will be defining some terms and classifications of hypertension in pregnancy.
#30 Hypertension is defined as having a systolic BP of >/= 140 or a diastolic bp of >/= 90. In pregnancy, hypertensive disorders are defined as the same value but they differ in the timing of diagnosis as well as the clinical manifestations.
Proteinuria is having the presence of protein in the urine. More specifically, the criteria we’re looking for includes a >/= 300mg/24 hr urine collection, urine protein/creatinine ratio of >/= 0.3, and a 1+ result in urine dipstick test.
Gestational hypertension is defined as having a bp of ≥ 140/90 on 2 occasions at least 4 hours apart after 20 weeks AOG or within 12 weeks postpartum without proteinuria or any organ dysfunction
#31 Now for pre eclampsia, this is defined as having a BP > ≥140/90 on 2 occasions at least 4 hours apart after 20 weeks AOG with proteinuria OR presence of
Thrombocytopenia: defined as having a plt ct of <100,000/uL
renal insufficiency: crea > 1.1 dL or 2x baseline
Liver involvement reflected by increase in AST, ALT 2x the normal value
Cerebral symptoms such as headache, visual disturbances, convulsions
Pulmonary edema
It can be further classified into either preeclampsia with severe features or preeclampsia without severe features
It is classified as severe if if one or more of the ff is present: severe hypertension ( ≥ to 110 diastolic, 160 systolic), oliguria, increase serum creatinine, congestive HF, Pulmonary edema, persistent headache, visual disturbance thrombocytopenia, hepatic/RUQ pain, elevated liver enzymes, renal abnormality
#32 Eclampsia is like preeclampsia but with the presence of generalized seizure not attributed to other causes.
Chronic hypertension is having having hypertension even before pregnancy or before the 20th week of gestation
#33 Lastly, chronic hypertension with superimposed pre eclampsia is defined as pre eclampsia with preexisting chronic hypertension. This condition occurs when chronic hypertension leads to worsening high blood pressure during pregnancy. This having a new-onset proteinuria meaning no proteinuria < 20 wks AOG or sudden increase in proteinuria or in BP (if with proteinuria <20 wks AOG) or thrombocytopenia (if with proteinuria <20 wks AOG)
Compared with “pure” pre-eclampsia, superimposed preeclampsia commonly develops earlier in pregnancy and tends to be more severe and more often accompanied by fetal-growth restriction.
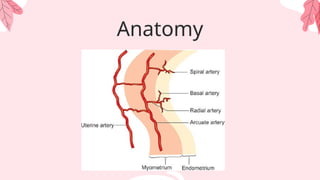
#35 here we have the anatomy of the uterine circulation. The blood supply of the uterus is provided by the uterine and ovarian arteries. These then branch off to become arcuate and radial arteries on the myometrium. And branches off as the spiral arteries then arterioles on the endometrium, which becomes in direct contact with the placenta.
#36 -During normal pregnancy, the villous cytotrophoblast invade through the myometrium and the decidua to gain access and infiltrate the spiral arteries. They then invade the endothelium and the tunica media of the spiral arteries. These spiral arteries dilate and become low resistance blood vessels to facilitate blood flow to the placenta. A process in which we call “remodeling”
-Remodelling usually takes place in the late first trimester and is completed by 18 to 20 weeks of gestation
-In preeclampsia, the cytotrophoblast cells infiltrate the decidual portion of the spiral arteries, but fail to penetrate the myometrium. And the spiral arteries remain narrow, and unable to accommodate the increase in blood flow that can lead to placental hypoperfusion
(Karumanchi, S., Lim, K., & August, P. (2022). Preeclampsia: pathogenesis. UpToDate. Retrieved January 22, 2022, from https://www.uptodate.com/contents/preeclampsia-pathogenesis?search=preeclampsia&source=search_result&selectedTitle=5~150&usage_type=default&display_rank=5#H3)
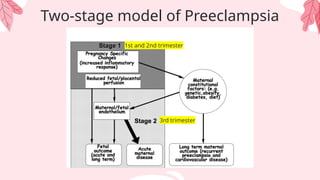
#37 We have what we call a Two Stage Model of Preeclampsia that emphasizes, a reduced placental perfusion on Stage 1 (or during the 1st and 2nd trim) is not sufficient to cause preeclampsia but requires interaction with maternal constitutional factors that may be genetic, behavioral or environmental. These factors are modified by the maternal pathophysiological changes of preeclampsia that results to maternal syndrome or the presence of maternal clinical manifestation
So during stage 1 of pre-eclampsia on the 1st and 2nd trimester, an interplay between risk factors, abnormal placentation, and an increase in anti-angiogenic factors, soluble Flt1 and soluble endoglin which are secreted by the placenta, are responsible for the clinical manifestation of the disease. And Stage 2 is when there is already presence of maternal clinical manifestation leading to Maternal syndrome. Which will be discussed further on the next slide
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2680383/
Included to from last week’s chairman’s lecture, add ko na lang din –Alix
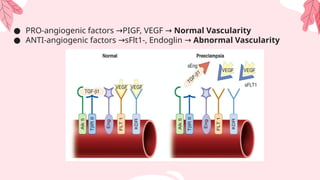
#38 During stage 1, Proangiogenic factors Vascular endothelial growth factor (VEGF) and placental growth factor (PIGF) are important in the stabilization of endothelial cells in mature blood vessels needed for normal vascularity. Whereas Blockade of both VEGF and PlGF due to soluble Flt1 and soluble endoglin leads to an abnormal vascularity.
Here we can see that VEGF and PIGF are present in normal pregnancy, whereas sFlt-1 and endoglin inactivate and reduce circulating free placental growth factor (PlGF) and VEGF concentrations, leading to endothelial dysfunction resulting in hypertension, proteinuria, and the other systemic manifestations of preeclampsia.
Chairman’s rounds and https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3063446/#:~:text=Soluble%20Flt1%20and%20soluble%20endoglin,other%20systemic%20manifestations%20of%20preeclampsia.
#39 To elaborate further on the pathophysio of preeclampsia, Immunologic intolerance between the mother and fetus may play a role in the pathogenesis of pre-eclampsia. Excessive production of immune cells causes secretion of tumor necrosis factor alpha, which incites apoptosis of extravillous cytotrophoblasts. Reduced levels of HLA-G and HLA-E seen in women with preeclampsia may also play a factor in the defective invasion of spiral arteries. In normal pregnancies, the interaction between these cells and the trophoblast is caused by the secretion of vascular endothelial growth factor and placental growth factor by natural killer cells.
#40 [Preeclampsia is caused by the abnormal development of placental vasculature and maternal systemic endothelial dysfunction]. –already mentioned!!
Now we look at the effects that preeclampsia has on the fetus, on the mother, and on the placenta.
Fetal effects due to abnormal placentation: causes uteroplacental insufficiency leading to IUGR and hypoxia
Maternal effects are due to the circulating anti-angiogenic factors which leads to increased vascular permeability, coagulation activation, vasoconstriction. This results in end-organ damage manifested as:
Seizure and stroke
Oliguria and renal failure
Pulmonary edema
Edema and subcapsular hematoma of the liver
Thrombocytopenia and disseminated intravascular coagulation
These will be further discussed in the following slides.
Placental effects - placental vessels should be dilated (term called ballooning). When constricted, tunica media is retained → no ballooning → increase in blood pressure. Pro angiogenic > antiangiogenic
Defective invasion of spiral arteries by cytotrophoblasts leads to increased uterine arterial resistance, inducing higher sensitivity to vasoconstriction, and thus chronic placental ischemia and oxidative stress
#41 During normal pregnancy, renal blood flow and glomerular filtration rate are increased appreciably. But with development of preeclampsia, there may be decreased renal perfusion and glomerular filtration. So in preeclampsia, you have the reverse. This is because the blood is preferentially shunted to the mother’s brain, lungs and heart. The kidney is not prioritized, thus resulting in decreased renal perfusion
As we see in this diagram there is renal hypoperfusion resulting to a decrease in GFR, and ischemia to renal tissues. A decrease in GFR causes oliguria, and an increase in BUN, creatinine, and uric acid. Ischemia to renal tissues causes proteinuria due to increased tubular permeability. This leads to dec. intravascular oncotic pressure, increased hydrostatic pressure resulting to edema. This can also result to a decrease in serum albumin and increased urine protein.
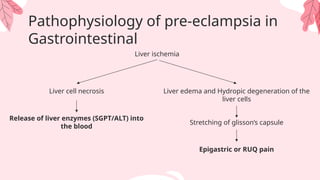
#42 Hemodynamic changes during pregnancy include a progressive increase in CO and a decrease in the systemic vascular resistance leading to a high-volume, low-resistance circulation.
But in preeclampsia, there is increased peripheral resistance leading to increased afterload from higher vascular resistance created by impaired placentation would lead to a left sided heart failure. Congestive heart failure may lead to pulmonary edema when the heart is not able to pump efficiently, blood can back up into the veins that take blood through the lungs. As the pressure in these blood vessels increases, fluid is pushed into the air spaces (alveoli) in the lungs
Expect: increased BP and increased HR
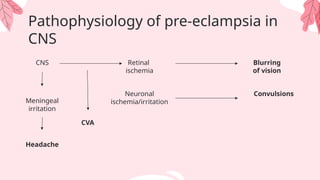
#44 Headaches are thought to be reflective of elevated cerebral perfusion pressure, cerebral edema, or hypertensive encephalopathy. Headache may be temporal, frontal, occipital, or diffuse. It may be caused be general endothelial cell dysfunction, which results in vasospasm of cerebral vasculature in response to severe hypertension or loss of cerebral autoregulation, leading to areas of vasoconstriction and vasodilation.
Visual symptoms can be caused by retinal arteriolar spasm, impaired cerebrovascular autoregulation, and cerebral edema.
August, P., & Sibai, B. (2023). Preeclampsia: Clinical features and diagnosis. UpToDate. Retrieved January 22, 2023 from https://www.uptodate.com/contents/preeclampsia-clinical-features-and-diagnosis?search=preeclampsia&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1#H3583231095
American College of Obstetricians and Gynecologists (2020). Gestational Hypertension and Preeclampsia. Obstetrics & Gynecology, 135(6), e237–e260. doi:10.1097/aog.0000000000003891
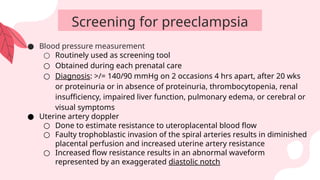
#46 All pregnant women should be screened for preeclampsia between 11 weeks to 13 6/7 weeks using maternal risk factors and biomarkers. Maternal risk factors were mentioned earlier. Biomarkers include:
Blood pressure measurement
It is a Routinely used as screening tool which can be Obtained during each prenatal care
Diagnosis: >/= 140/90 mmHg on 2 occasions 4 hrs apart, after 20 wks or proteinuria or in absence of proteinuria, thrombocytopenia, renal insufficiency, impaired liver function, pulmonary edema or cerebral or visual symptoms
Uterine artery doppler
This is a measurement of uterine artery blood flow velocity used to estimate resistance to uteroplacental blood flow.
As discussed, faulty trophoblastic invasion of the spiral arteries results in diminished placental perfusion and upstream increased uterine artery resistance. Increased uterine artery velocimetry determined by Doppler ultrasound in the first two trimesters should provide indirect evidence of this process and thus serve as a predictive test for preeclampsia. Increased flow resistance results in an abnormal waveform represented by an exaggerated diastolic notch
#47 Roll Over Test
This is recommended as routine test for every patient between 28-32 weeks gestation which can be done in the outpatient or in primary care setting. It measures the hypertensive response by comparing the BP from resting in the left lateral decubitus position then roll over to the supine position. The roll-over test is considered positive if the diastolic blood pressure increased 20 mmHg or more in dorsal decubitus (supine), with respect to that obtained in lateral decubitus, at 1 minute and at 5 minutes.
For healthy vessels, levels of pro angiogenic factors (PIGF and VEGF) should be greater than anti angiogenic factors (soluble fms-like tyrosine kinase-1 , soluble endoglin). Angiogenic imbalance is used to describe excessive amounts of antiangiogenic factors hypothesized to be stimulated by worsening hypoxia at the uteroplacental interface.
Increased maternal sFlt-1 levels inactivate and decrease circulating free PlGF and VEGF concentrations, leading to endothelial dysfunction. SFlt-1 levels can be measured which begin to increase in maternal serum months before preeclampsia while high levels in the second trimester were associated with a doubling of the risk for preeclampsia
#51 Low dose aspirin for preeclampsia prevention is recommended for patients with two or more of the following moderate risk factors: Nulliparity, Obesity (body mass index >30 kg/m2), Family history of preeclampsia in mother or sister, Age ≥35 years, Sociodemographic characteristics (Black persons, lower income level [recognizing that these are not biological factors]), Personal risk factors (eg, previous pregnancy with low birth weight or small for gestational age newborn, previous adverse pregnancy outcome [eg, stillbirth], interval >10 years between pregnancies)., In vitro conception
Low dose aspirin should be given At 60-150 mg/day at night starting at 11-14 weeks gestation or <16 weeks until 36 weeks AOG, it diminishes platelet thromboxane synthesis while maintaining vascular wall prostacyclin synthesis. Low dose aspirin also modulates inflammation which is exaggerated in patients with preeclampsia.
As for the calcium supplementation, WHO recommends 1500-2000 mg elemental calcium supplementation per day for pregnant individuals. Increased hydration is advised to prevent urolithiasis.
Other preventive strategies would be to have exercise and to take antioxidants such as ascorbic acid and vitamin D.
#52 For the definitive treatment, The ultimate management of preeclampsia is the Delivery of the baby
To improve maternal outcomes, delivery is generally indicated at 37 weeks' gestation for women who have preeclampsia without severe features to treat the preeclampsia and prevent further complication. immediate delivery between 34 weeks and 36 weeks and six days is not recommended because of an increase risk of neonatal respiratory distress syndrome.
For patient with preeclampsia without severe features at GA of less than 37, Expectant management of preeclampsia may include BP monitoring, weekly laboratory tests (complete blood count and monitoring of creatinine levels, alanine transaminase, and/or aspartate transaminase levels), fetal nonstress testing, weekly amniotic fluid indices, and fetal growth ultrasonography
—---------------
Patient with severe signs with AOG of less than 37. They will require hospitalization for careful monitoring. Treatment goals are fluid management, seizure prevention, lowering BP to prevent maternal end-organ damage, and expediting delivery based on disease severity and gestational age in an attempt To deliver a healthy newborn. Delivery may be done after maternal stabilization
If Patient is with severe signs and the fetus is Between 24 and 34 weeks' of gestation, delivery of the baby should be deferred and given corticosteroids. And Reassessment of conservative management after 24hrs should be done. fetal lung maturity may be accelerated by the use of betamethasone (two 12-mg intramuscular doses given 24 hours apart) or dexamethasone (four 6-mg intramuscular doses given 12 hours apart)
Antenatal testing in women who have preeclampsia with severe features may include daily nonstress tests, amniotic fluid assessment, and periodic ultrasonography to assess fetal growth.
#54 For the control of convulsions of those with preeclampsia without severe features. The patient should be monitored closely, and magnesium sulfate (MgSO4) are not recommended and should only be started if severe features develop. Symptoms such as Severe headache, visual disturbances, and hyperreflexia may signal impending eclamptic seizure
magnesium sulfate (MgSO4) can help in the prevention of eclamptic seizures and placental abruption in women who have preeclampsia with severe features.and It is more effective when compared to other anti seizure medication such as phenytoin, or diazepam.
Magnesium is a calcium antagonist which can act on most calcium channels. It decreases intracellular calcium which causes arterial relaxation and subsequently, cerebral vasodilation. This aids in the cerebral vasospasm that happens during convulsions.
magnesium sulfate is administered intravenously, This is given during labor or when the decision to deliver the baby is made, and up to 24 hours postpartum. This will be further explained on the next slide
—--------------------
MgSO4 treatment must be monitored in the intensive care unit because organ failure may occur. This monitoring is based on repeated checking for a.) Absent Deep Tendon Reflexes. b) Respirations less than 12/minute, shortness of breath, or respiratory arrest. c) Chest pain d) Urinary output less than 30 ml /hour. e) A significant drop in pulse or BP. f) Signs of fetal distress. g) Coma.
Antidote for Magnesium sulfate toxicity is Calcium gluconate.
#55 So for intrapartum management, we may use ripening agents such as Dinoprostone or Prostaglandin E2, as in our patient and oxytocin, also used in our patient’s case. But we should take note of some factors such as (read). So in our patient, we saw that after 3 doses of Dinoprostone, the IE remained the same and after 4 hours of induction of labor, the fetus had a non-reasurring heart rate and status with persistent variable decelerations noted, which warranted the CS delivery.
For control of hypertension, hydralazine, labetalol or methyldopa may be given. In our patient, Hydralazine 15mg IV was used as well as 2 tablets Methyldopa 250mg/tab every 6 hours.
For fluid management, NSS is usually recommended at a rate of 80cc/hr.
For seizure prophylaxis, we have usually start with a loading dose of 4-6g of Magnesium SUlfate, in our case we used 4g for our loading dose. Maintenance infusion rate is recommended to be 1-2g/hr, we used 1g for our patient.
So a contraindication we hsould take note of is myasthenia gravis, so in patient with this condition, the already damaged nerve-muscle connections may be worsened by the magnesium sulfate which as blocker of calcium-mediated contractions and so in these patients, other anti-seizure medications such as leveteracitam may be used.
#57 ACOG (2022) recommends utilizing 140/90 as the threshold for initiation or titration of medical therapy for chronic hypertension in pregnancy, rather than the previously recommended threshold of 160/110
Antihypertensive medications safe for treatment of hypertension during pregnancy include:
Methyldopa, two or three times daily up to 3,000 mg per day
Labetalol, two times daily up to 2,400 mg per day in women without asthma, myocardial disease, decreased cardiac function, heart block, or bradycardia;
Extended-release nifedipine, up to 120 mg daily in women without tachycardia;
Hydrochlorothiazide, 12.5 to 25 mg daily.
Methyldopa is the drug of choice for chronic hypertension in pregnancy. Other medications have side effects, such as fetal growth restriction in labetalol, and volume contraction and electrolyte disorders for hydrochlorothiazide.
Use of angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, renin inhibitors, and mineralocorticoid receptor antagonists should be avoided in pregnancy.
#58
Obtain baseline laboratory work-ups such as complete blood count, complete metabolic panel, and baseline 24-hour urine for creatinine clearance and protein
Obtain baseline ECG to ensure no current cardiac compromise
Initiate low-dose aspirin after 12 weeks to reduce risk of superimposed preeclampsia

























![PIHTN.pptx is increase of blood pressure during pregnancy of the mother [{}]#...](https://cdn.slidesharecdn.com/ss_thumbnails/pihtn-240806061903-454708ae-thumbnail.jpg?width=640&height=640&fit=bounds)

































